
Emergency Medicine
Session: Emergency Medicine 4

Andrea Rivera-Sepulveda, MD, MSc
Associate Professor
Nemours Children's Hospital
ORLANDO, Florida, United States
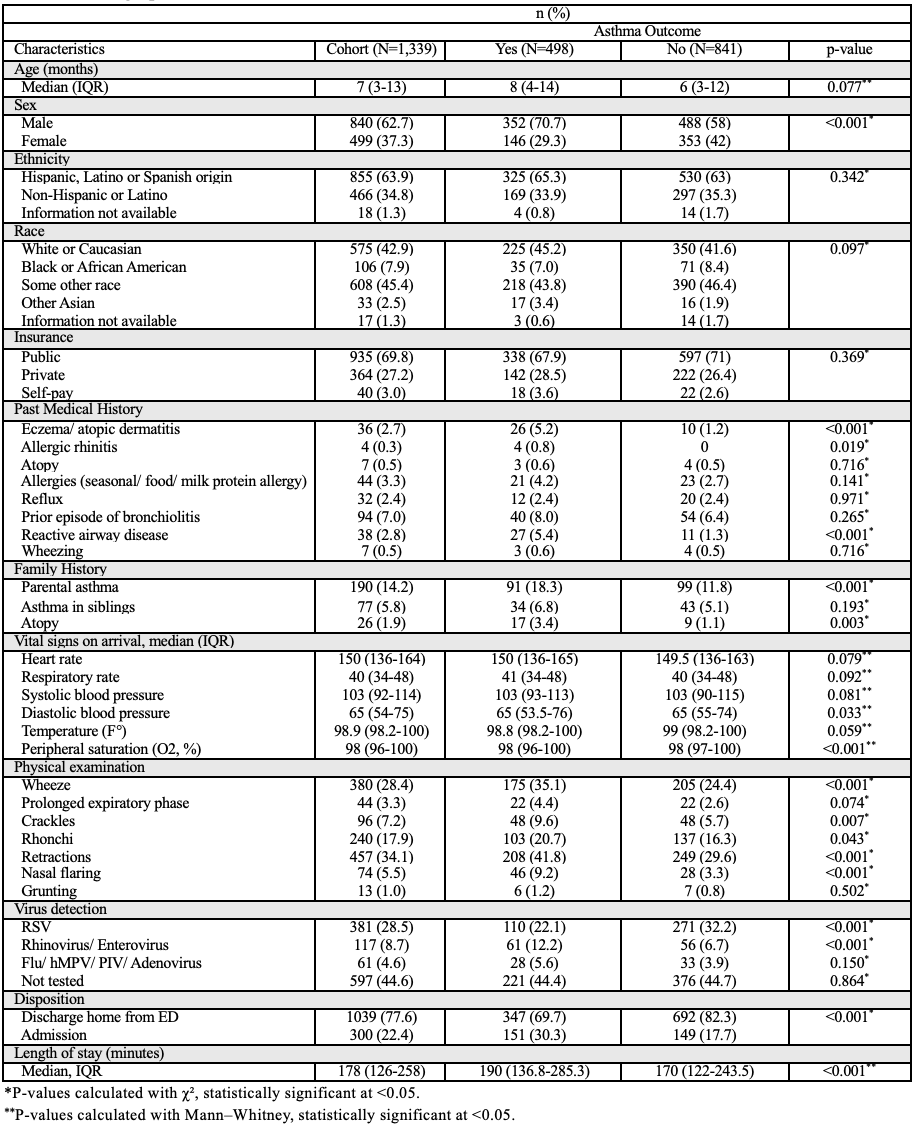 Notes: Values shown as n (%) unless specified. p-values from χ² or Mann-Whitney, as appropriate. Table shows that children who later developed asthma already had more airway/atopic features and a different viral pattern at the index visit.
Notes: Values shown as n (%) unless specified. p-values from χ² or Mann-Whitney, as appropriate. Table shows that children who later developed asthma already had more airway/atopic features and a different viral pattern at the index visit.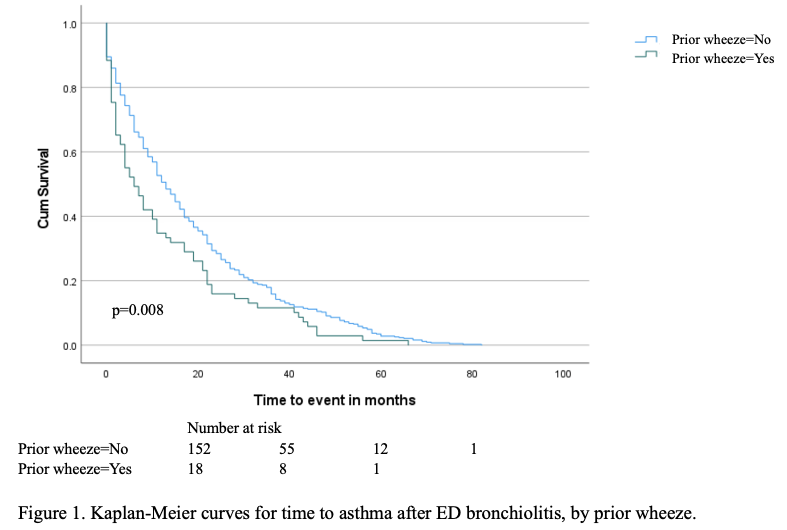 Time from index bronchiolitis ED visit to first asthma diagnosis. Children with documented prior wheeze had a markedly lower asthma-free survival at 24 months (0.159 → 84.1% with asthma) compared with those without prior wheeze (0.284 → 71.6% with asthma); log-rank p = 0.008.
Time from index bronchiolitis ED visit to first asthma diagnosis. Children with documented prior wheeze had a markedly lower asthma-free survival at 24 months (0.159 → 84.1% with asthma) compared with those without prior wheeze (0.284 → 71.6% with asthma); log-rank p = 0.008.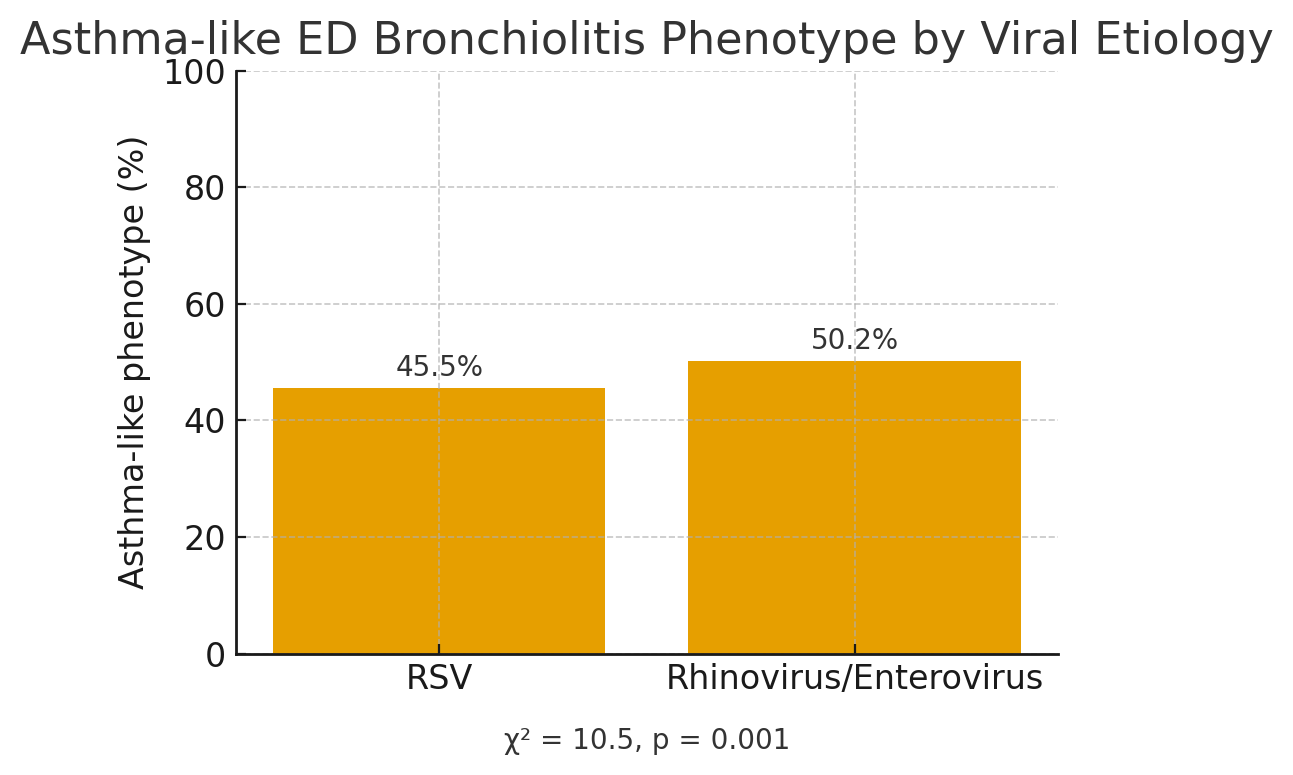 Figure 2. Proportion of ED bronchiolitis encounters classified as asthma-like (defined as ≥1 of: prior wheeze, ED bronchodilator or systemic steroid, airway/wheeze/RAD ED diagnosis, or atopy history) by viral etiology. Children with rhinovirus/enterovirus were more often asthma-like than those with RSV (50.2% vs 45.5%; χ²=10.5, p=0.001), supporting an RV-triggered, asthma-prone bronchiolitis phenotype.
Figure 2. Proportion of ED bronchiolitis encounters classified as asthma-like (defined as ≥1 of: prior wheeze, ED bronchodilator or systemic steroid, airway/wheeze/RAD ED diagnosis, or atopy history) by viral etiology. Children with rhinovirus/enterovirus were more often asthma-like than those with RSV (50.2% vs 45.5%; χ²=10.5, p=0.001), supporting an RV-triggered, asthma-prone bronchiolitis phenotype.