645 - Gestational Age Specific Mortality in infants 33-42 weeks Receiving Therapeutic Hypothermia: A report from the Children's Hospitals Neonatal Consortium
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2629.645
Jeffrey Shenberger, Connecticut Children's, Hartford, CT, United States; Isabella Zaniletti, IZ Statistics LLC, Tampa, FL, United States; Robert DiGeronimo, Seattle Children's, Seattle, WA, United States; Girija Natarajan, Central Michigan University College of Medicine, Detroit, MI, United States; Ulrike Mietzsch, University of Washington School of Medicine/ Seattle Children's Hospital, Seattle, WA, United States; Swetha Padiyar, Wake Forest Baptist Health - Brenner Children's Hospital, Winston- Salem, NC, United States; Michael A.. Padula, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Theresa Grover, Children's Hospital Colorado, Aurora, CO, United States; Karna Murthy, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Mehmet Cizmeci, The Hospital for Sick Children, Toronto, ON, Canada; Jennifer A. Rumpel, University of Arkansas for Medical Sciences College of Medicine, Little Rock, AR, United States; Kelsey M. Sullivan, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States; Vonita Chawla, Arkansas Children's Hospital, Little Rock, AR, United States; Ryan M. McAdams, University of Wisconsin School of Medicine and Public Health, Middleton, WI, United States; Katsuaki Kojima, Cincinnati Children's Hospital Medical Center, Montgomery, OH, United States; Ceyda Acun, Cleveland Clinic Children's Hospital, Cleveland, OH, United States; Semsa Gogcu, Brown University, South Kingstown, RI, United States; Robert M. Dietz, University of Colorado School of Medicine, Aurora, CO, United States; Vilmaris Quinones Cardona, Drexel University College of Medicine, Philadelphia, PA, United States; Susan Cohen, CW HOPE Developmental Follow Up Clinic, Milwaukee, WI, United States; Eric S. Peeples, University of Nebraska Medical Center, Omaha, NE, United States; Maria L. V.. Dizon, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Rakesh Rao, Washington University in St. Louis School of Medicine, St. Louis, MO, United States
Professor Connecticut Children's Hartford, Connecticut, United States
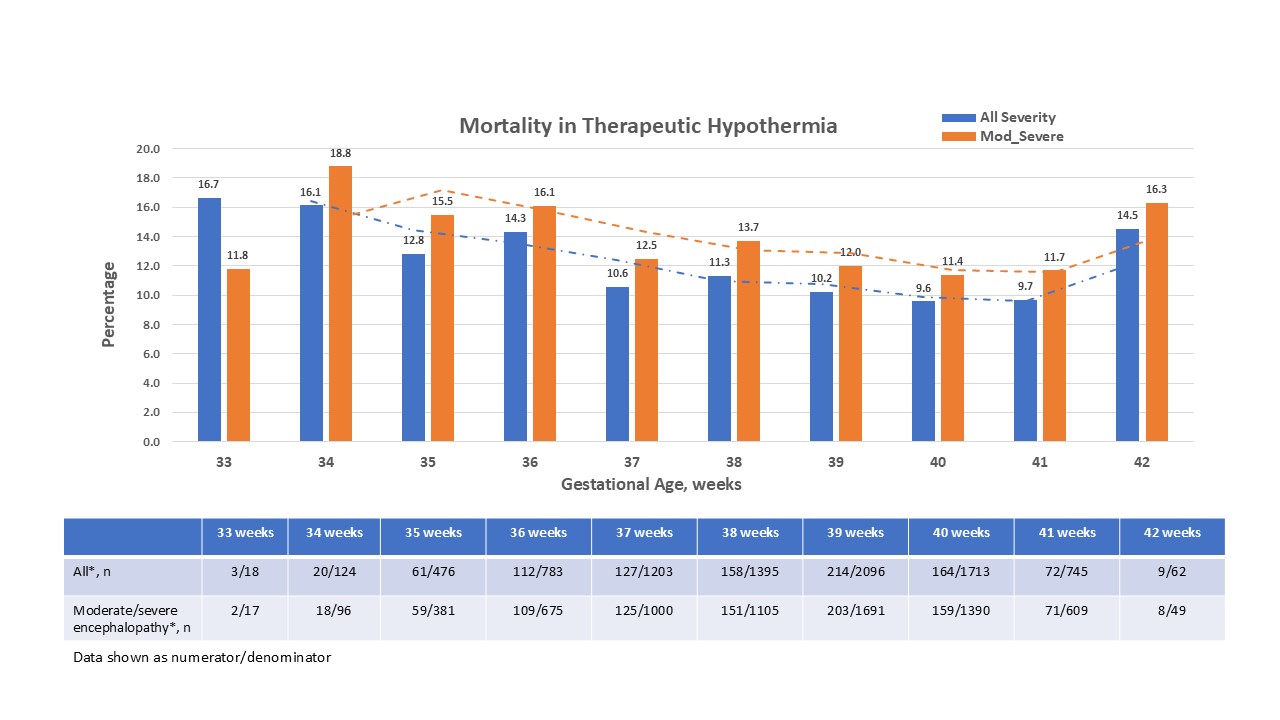
Background: Therapeutic hypothermia (TH) is standard management for infants with moderate- severe hypoxic-ischemic encephalopathy (HIE) born ≥ 35 weeks gestational age (GA). A recent trial of TH in infants 33-35 weeks GA with moderate or severe HIE suggested that hypothermia may increase death and discouraged using TH in this GA. Objective: To describe mortality and comorbidities by GA in infants undergoing TH for presumed HIE. Design/Methods: Data were collected from the CHNC database from 2010-2025. Infants 33-42 weeks GA with HIE or central nervous system depression treated with TH were categorized by the severity of encephalopathy (mild, moderate, severe, or unknown). Mortality was reported by GA week and demographic, perinatal, and neonatal variables grouped for infants 33-35 (preterm, PT) and 36-42 weeks GA (near term/term, NTT). Results: 8,615 infants 33-42 weeks GA underwent TH with 618 (7.1%) being PT. Demographic and perinatal data are listed in Table 1. PT had higher rates of maternal diabetes, hypertension, placental abruption, and Cesarean delivery (p < 0.001), but had less chorioamnionitis and small for gestation (p < 0.001). The groups differed by severity of encephalopathy (p=0.005). Moderate-severe encephalopathy occurred in 80% of PT and 81.5% of NTT infants. Mortality was 10.9% (940/8615) for all stages of encephalopathy; 2.1% (109/5159) in moderate and 42.9% (796/1854) in severe encephalopathy, respectively. Grouping by GA revealed that 13.6% of PT infants died compared to 10.7% at NTT (p=0.027). Age and cause of death did not differ between groups and redirection of care was seen in 89.1% PT and 89.3% NTT infants (Table 2). Mortality by GA week ranged from 9.6% at 40 weeks to 16.7% at 33 weeks GA for all grades of encephalopathy (Fig 1). Evaluating only moderate-severe HIE, mortality was lowest at 40 weeks (11.4%) and highest at 34 weeks GA (18.8%). The first MRI at a CHNC site for reported infants was abnormal in 60.6% (243/401) in PT vs. 53.1% (2686/5061) in NTT (p < 0.001). Subdural hemorrhage occurred less often (10.5% vs. 17.6%, p< 0.001) and intraventricular hemorrhage more often (22.9% vs. 9.1%, p=0.044) in PT infants. Parenchymal hemorrhage (33.4% vs. 28.6%), white matter injury (44.4% vs. 32.2%), deep nuclear gray (22.7% vs. 20.4%) and cortical injury (11.5% vs. 12.6%) did not differ.
Conclusion(s): Mortality was higher in PT compared to NTT and varied by GA week in infants treated with TH. Differences in perinatal and neonatal events may contribute to encephalopathy and MRI findings. Additional analyses are ongoing
Table 1. Selected Demographic and perinatal variables of infants treated with Therapeutic Hypothermia (TH) stratified into 33-35 weeks and 36-42 weeks gestational age (GA). SGA = small for gestational age.
Table 2. Mortality associated variables of infants dying following Therapeutic hypothermia (TH) stratified into 33-35 weeks and 36-42 weeks gestational age (GA). N (%) or median [25th, 75th percentile]; DNR = do not resuscitate; CPR: cardiopulmonary resuscitation; BSI = blood stream infection.
Figure 1: Mortality by GA for all severity (blue) and in moderate or severe encephalopathy (orange) treated with Therapeutic Hypothermia.

 photo")
.jpg)
.jpg)