418 - Radiographic Monitoring in Pediatric Osteomyelitis: Impact on Care
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2406.418
Danielle S.. Comeaux, Texas Children's Hospital & Baylor College of Medicine, Woodlands, TX, United States; Jonathon Chase. McNeil, Baylor College of Medicine, Houston, TX, United States; Nicole Wunderlich, Texas Children’s Hospital, Tomball, TX, United States; ankhi Dutta, Baylor College of Medicine, Spring, TX, United States; Holly Oliver, Texas Children's Hospital, The Woodlands, TX, United States; Megan James, Texas Children's Hospital, The Woodlands, TX, United States; Shannen Humphrey, Texas Children's Hospital, Spring, TX, United States
Associate Professor Baylor College of Medicine Spring, Texas, United States
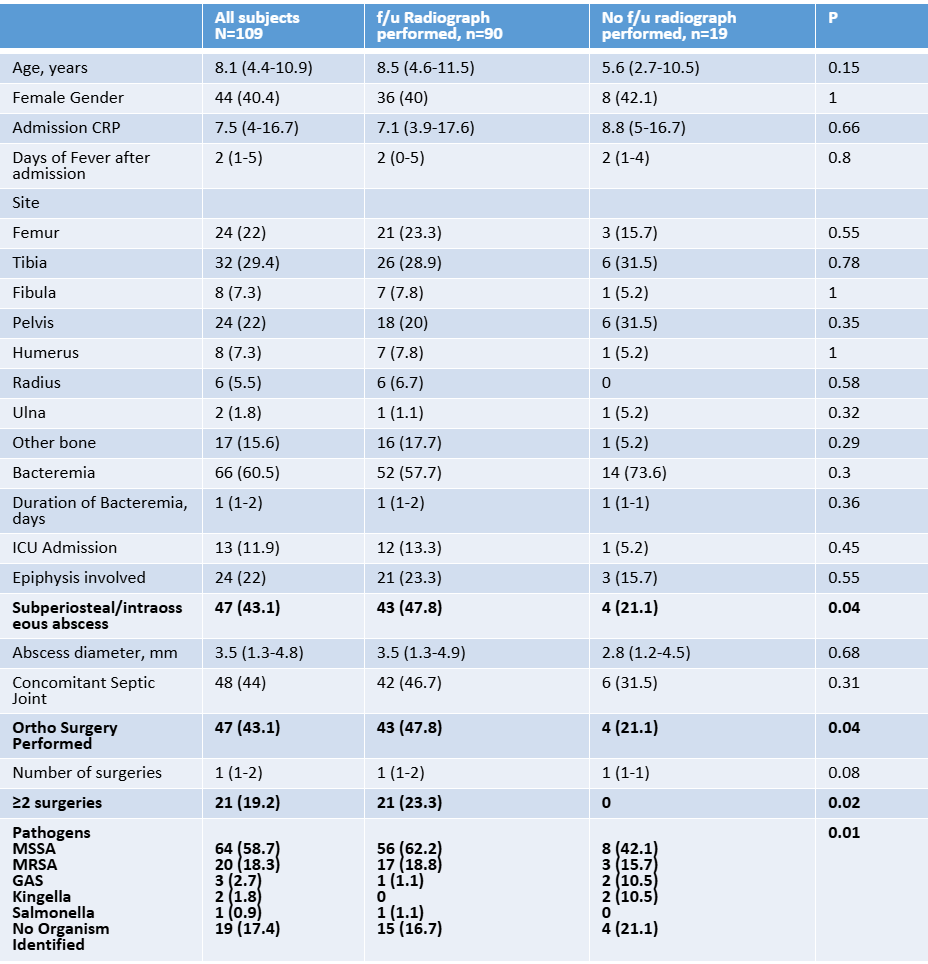
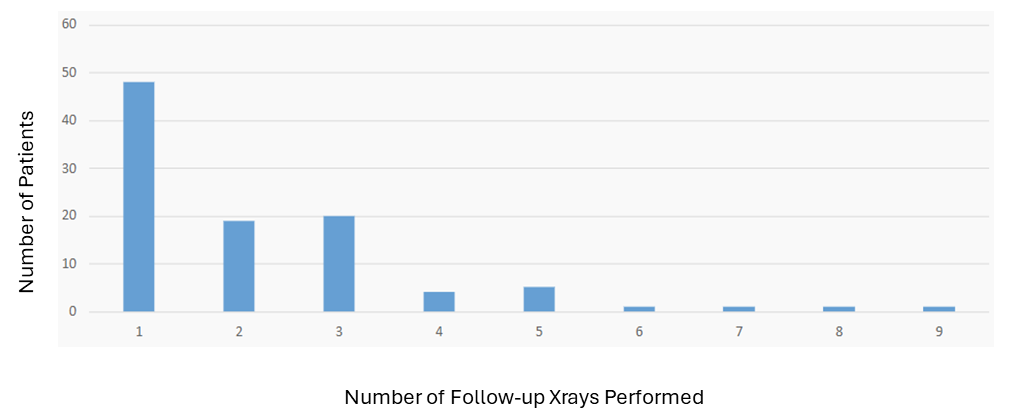
Background: Pediatric acute hematogenous osteomyelitis (AHO) and septic arthritis (SA) are significant causes of morbidity, accounting for ~1.8 per 1,000 emergency department visits annually. The clinical impact of follow-up radiographs in AHO and SA is uncertain. The Pediatric Infectious diseases clinical practice guidelines suggest follow-up radiographs for complicated AHO or if there is physeal involvement, although evidence is limited to support this. Objective: The primary objective of this study was to assess whether end of therapy radiological findings influence medical or surgical management in pediatric AHO. A secondary objective was to evaluate whether infection site and/or physeal involvement affect radiograph use and clinical outcomes. Design/Methods: This IRB-approved retrospective observational study included pediatric patients (0-18 years) admitted with AHO to a U.S. quaternary care hospital from 2015 to 2022. Patients were identified via ICD-9/10 codes and confirmed by imaging. Data on demographics, clinical presentation, labs, microbiology, imaging, treatment, and outcomes were extracted from electronic medical records. Results: 109 patients met inclusion criteria. Median age was 8.1 years (IQR: 4.4-10.9); 40.4% were female. The tibia was the most affected site (29.4%), and 22% had epiphyseal involvement. Concomitant SA occurred in 44%. Methicillin-sensitive Staphylococcus aureus (MSSA) was the most common pathogen (58.7%). Follow-up radiographs were obtained in 82.6% (Table I) more frequently performed in those with osseous abscesses and/or surgical interventions. The median number of radiographs per subject was 1 (IQR: 1-3) (Graph I). Rates of radiography were similar regardless of site of disease or epiphyseal involvement. The median time from index admission to first follow-up radiograph was 31.5 days (IQR: 22-61). Among clinically improved patients who underwent radiography (n=85), only 1.2% had concerning findings. In contrast, in patients with persistent or worsening symptoms (n=5), 60% had radiographs showing concerning pathology necessitating change in management.
Conclusion(s): Radiographs are frequently used in follow up care for pediatric AHO and SA, especially in more severe cases or those requiring surgery. Follow-up radiographs rarely change clinical management in patients with clinical improvement. These findings support reevaluating routine radiographic follow-up to optimize care and resource use.
Table I: Demographics and Radiograph Utilization
Table II: Correlation Between X-Ray Findings and Clinical Outcomes
Graph I: Frequency of Follow-Up X-Rays Performed in Patient Cohort