548 - Adherence to Antibiotic Prescribing Guideline Recommendations for Febrile Young Children in the Pediatric Emergency Department (ED)
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2533.548
Kelly Peterec, Yale-New Haven Children's Hospital, New Haven, CT, United States; Emily Powers, Yale School of Medicine, New Haven, CT, United States; Rakesh D. Mistry, Yale School of Medicine, New Haven, CT, United States
Medical Student Yale School of Medicine New Haven, Connecticut, United States
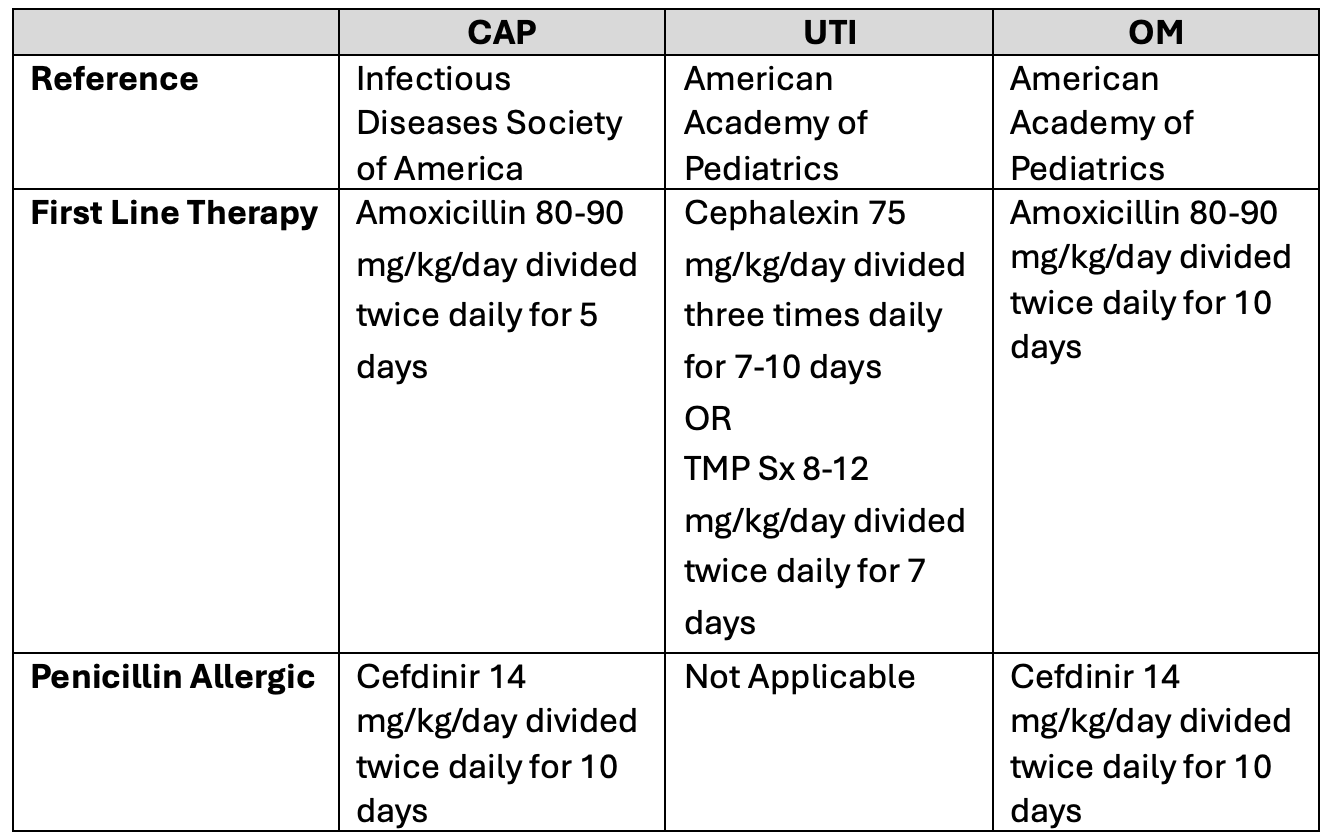
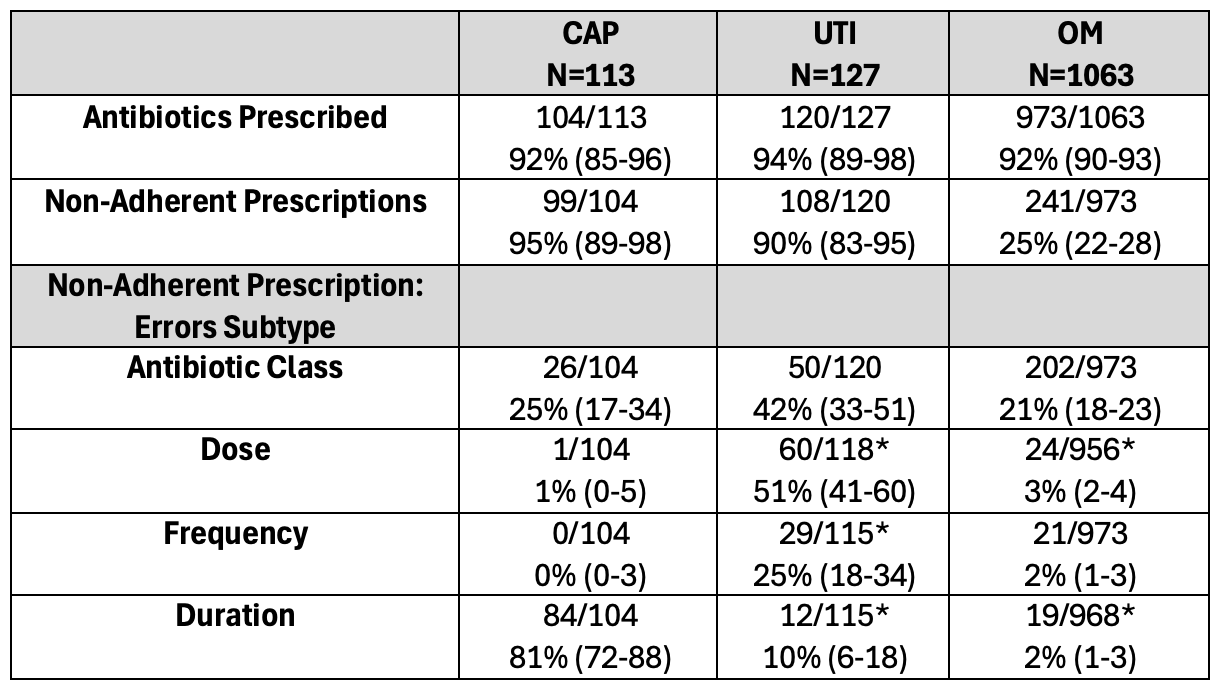
Background: Recommended prescribing guidelines exist for common ED infections including community acquired pneumonia (CAP), otitis media (OM), and urinary tract infections (UTI). Failure to adhere to prescribing guidelines contributes to excessive antibiotic exposure and promotes development of antimicrobial resistance. Objective: To evaluate adherence with established antibiotic prescribing guidelines for CAP, OM, and UTI in febrile young children treated in the pediatric ED. Design/Methods: We performed a retrospective review of children aged 2-36 months with fever (≥38ºC) or chief complaint of fever treated and discharged from a tertiary-care pediatric ED from 2022-2024. Using ICD-10 codes, we identified ED visits of children discharged with antibiotic prescriptions for CAP, OM, or UTI. Visits with multiple bacterial infections were excluded. Visit details, demographics, and antibiotic prescriptions were collected. Discharge antibiotic prescriptions were compared with nationally recommended guidelines for each infection (Table 1). Error subtypes, including antibiotic class, dose, frequency and duration, were determined. From 10/2022-4/2023 a nationwide amoxicillin shortage impacted antibiotic availability; we assessed the relationship between the shortage on prescribing errors. Results: Among 8026 febrile children, 1197 met study criteria. Antibiotics were prescribed for 104/113 (92%) patients with CAP, 120/127 (94%) with UTI, and 973/1063 (92%) with OM. Overall, prescribing errors occurred in 448/1197 (37.4%; 95% CI 34.7-40.2) of visits with antibiotics prescribed. Prescribing errors were observed for all three infections, and most frequent for CAP (95%) and UTI (90%); OM (25%) had the lowest rate of prescribing errors (Table 2). Errors due to prescribing broad-spectrum antibiotics such as third-generation cephalosporins or amoxicillin-clavulanate were frequent (30.0%; 95% CI: 27.4-32.7), and most common in UTI (38%) and OM (20%). Among prescribing error subtypes, the highest rate was for CAP antibiotic duration with 81% prescribing >5 days. Dosing and frequency errors were common for cephalexin in the treatment of UTI. Prescribing errors for OM were significantly impacted by the amoxicillin shortage (OR 3.9 95% CI 2.9-5.3) but were not associated with CAP or UTI.
Conclusion(s): ED antibiotic prescribing for common infections in febrile young children is frequently non-compliant with guidelines. Efforts to improve ED antimicrobial stewardship should emphasize use of narrow spectrum antibiotics for CAP and OM, appropriate duration of therapy for CAP, and correct frequency and dosing of cephalexin for UTI.
Table 1: Guidelines for Antibiotic Prescribing
Table 2: Analysis of Prescribing Errors *Denominators may differ as a result of missing data; 95% Confidence Interval in Parentheses

 *Denominators may differ as a result of missing data; 95% Confidence Interval in Parentheses
*Denominators may differ as a result of missing data; 95% Confidence Interval in Parentheses