119 - Comparison of Short Versus Long Courses of Erythropoietin Therapy in Preterm Infants in the NICU
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2114.119
Sevde B. Alptekin, 107511, Brooklyn, NY, United States; Akila M. Antony, New York Presbyterian Brooklyn Methodist Hospital, Brooklyn, NY, United States; Cecilia Ampem - Darko, New York Presbyterian Brooklyn Methodist Hospital, Brooklyn, NY, United States; Oksana Nulman, Weill Cornell Medicine, Brooklyn, NY, United States; Abhinav Parikh, NewYork-Presbyterian Komansky Children’s Hospital, Brooklyn, NY, United States; Humayun Shahzad, New York-Presbyterian Brooklyn Methodist Hospital, Brooklyn, NY, United States; Anna Pullicino, New York Presbyterian Brooklyn Methodist Hospital, Brooklyn, NY, United States; Samah A. Ahmed, NYP-Brooklyn Methodist Hospital, Jersey City, NJ, United States; Ali M. Nadroo, NYP Brooklyn Methodist Hospital, Brooklyn, NY, United States; Martin Dorciak, Weill Cornell Medicine, Brooklyn, NY, United States
Resident NYP- BMH Brooklyn, New York, United States
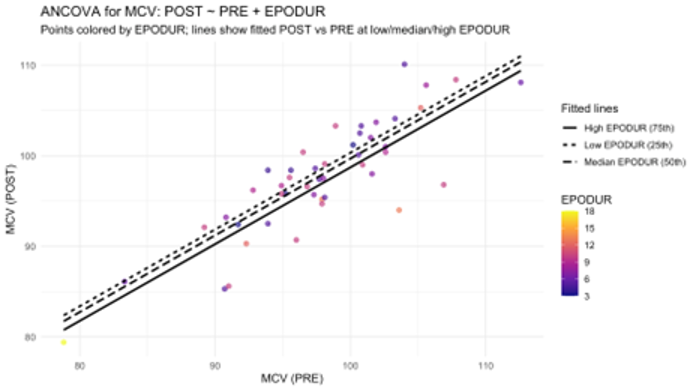
Background: Anemia of prematurity (AOP) is common in preterm infants, usually appearing between 2-6 weeks as normocytic, normochromic, hyporegenerative anemia. Causes include low endogenous erythropoietin (EPO), shortened red cell lifespan, and frequent phlebotomy, increasing transfusion needs, which carry risks of alloimmunization, infection, and iron overload. Recombinant EPO stimulates erythropoiesis and may reduce transfusions. Optimal therapy duration remains unclear, as prior studies report courses from two to nine weeks with inconsistent benefit beyond shorter regimens. Determining optimal length balances efficacy, safety, and cost. Objective: To compare hematologic, growth, and feeding outcomes in preterm infants receiving short ( < 8 days) versus long (≥8 days) EPO courses in the NICU. The 8-day threshold approximates the Neofax-recommended 10-day short course (300 U/kg/day SC) and reflects common early discontinuation or scheduling variation. Design/Methods: A retrospective chart review included 46 preterm infants with AOP admitted from January 2016 to August 2024 who received Epogen 300 U/kg/day SC. Infants with genetic abnormalities, congenital heart disease, prolonged respiratory support, or feeding difficulties affecting growth independently were excluded. Data collected included hemoglobin, hematocrit, reticulocyte hemoglobin, weight, feeding volume (mL/kg/day), and PO feeding percentage before and one week after therapy. Paired t-tests assessed pre-post changes; ANCOVA regression evaluated therapy duration effects; multiple regression analyzed growth. IRB approval was obtained. Results: Both short and long courses significantly increased hemoglobin, hematocrit, weight, and length (p < 0.01). Feeding volume improved significantly only in the ≥8-day group (p < 0.10), suggesting enhanced feeding tolerance. ANCOVA regression showed no independent effect of therapy duration on hematologic, growth, or feeding outcomes, except a modest negative association with mean corpuscular volume (p < 0.10). Shorter courses were modestly associated with greater length gain (+6%, p< 0.10). No adverse events were observed.
Conclusion(s): Extended EPO therapy may improve feeding tolerance but does not provide additional hematologic or growth benefits over shorter regimens. Outcomes likely reflect physiologic maturation rather than therapy duration. Future prospective and retrospective controlled studies-including EPO-treated, transfusion-only, and no-intervention groups-are needed to define optimal therapy length and clarify EPO's independent effects on hematologic response, feeding progression, and growth in preterm infants.