112 - The Bilirubin Screening Analysis in Very Preterm Infants (Biliscan) study:
A retrospective analysis on safety of in-hospital TcB screening in very preterm infants.
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2107.112
Frouke J. Terpstra, University Medical Center Groningen, Groningen, Groningen, Netherlands; Cornelia Betty Hendriksen, Children's Hospital, Nunspeet, Gelderland, Netherlands; Peter H. Dijk, Childrens, Groningen, Groningen, Netherlands; Elisabeth M.W.. Kooi, Beatrix Children's Hospital, University Medical Center Groningen, Groningen, Groningen, Netherlands; Jasper V. Been, Erasmus MC Sophia Children's Hospital, Rotterdam, Zuid-Holland, Netherlands; Christian V. Hulzebos, Beatrix Children's Hospital, University Medical Center Groningen, Groningen, Groningen, Netherlands
PhD-Candidate University Medical Center Groningen Groningen, Groningen, Netherlands
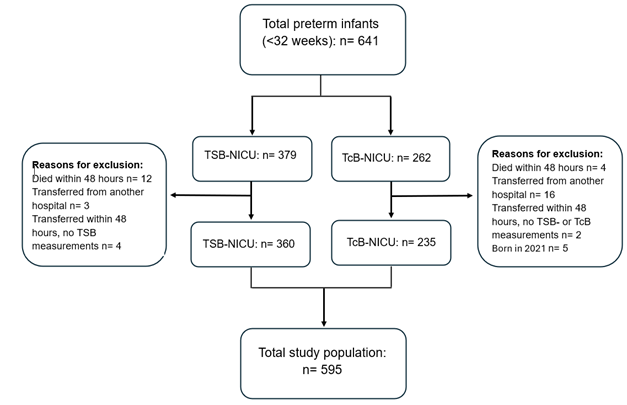
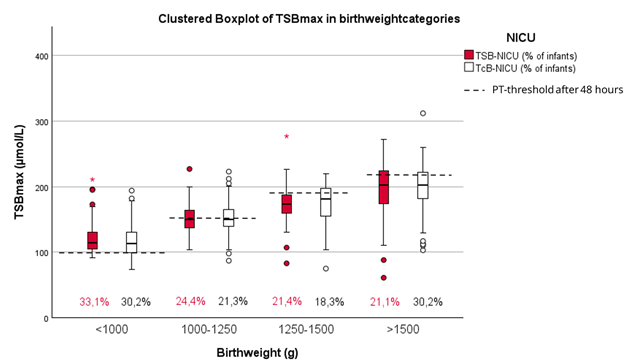
Background: Transcutaneous bilirubin (TcB) measurement is a reliable screening method for early detection of newborn infants > 35 weeks of gestation who need phototherapy. Yet, TcB screening is not routinely implemented in NICUs for very preterm infants. We hypothesized that TcB use in very preterm infants ( < 32 weeks) is safe and will reduce blood draws without increasing the maximum Total Serum Bilirubin (TSBmax). Objective: To determine if TcB screening reduces the number of invasive blood draws without increasing TSBmax. Design/Methods: We retrospectively analyzed data of preterm infants < 32 weeks admitted to two Dutch NICUs in 2022 and 2023. In NICU 1 bilirubin quantification was done without TcB screening. This 'TSB-NICU' used the ABL90FLEX PLUS (Radiometer Medical ApS, Copenhagen, Denmark) as TSB test instrument. In NICU 2, the 'TcB-NICU', standard TcB screening was performed, using the Dräger JM-105 (Dräger, Lübeck, Germany), and TSB quantification was done using a routine laboratory method (Roche Modular and Roche Cobas Pro, Roche Diagnostics, Mannheim, Germany) if TcB was ≥ 50 µmol above the corresponding national phototherapy threshold. Variables were analyzed with Student's t-test or Mann-Whitney U test, as appropriate; significance level was set at p < 0.05. Data are presented as median [IQR] unless stated otherwise. Results: Gestational ages and birth weights of included infants (Fig.1) were similar in both NICUs: 29 [27.5-30.5] weeks and 1177 [895-1458] grams in the TSB-NICU vs. 29 [27-31] weeks and 1220 [IQR 915-1525] grams in the TcB-NICU, respectively. The TSBmax was 151.0 [121-182] µmol/L in the TSB-NICU and 157.0 [120.0-194.0] µmol/L in the TcB-NICU (p=0.151). Figure 2 shows comparable TSBmax levels between the two NICUs across all different birthweight categories, that correspond to the national phototherapy (PT) threshold groups.
The number of TSB measurements was significantly lower in the TcB-NICU compared to the TSB-NICU (5 [3-7] vs. 9 [6-12], resp.; p< 0.001). Significantly more (+11,4%) preterm infants needed PT in the TSB-NICU than in the TcB-NICU (89,7% vs 78,3%, resp.; p< 0.001). PT was started earlier in the TSB-NICU compared to the TcB-NICU (40 [27.5-52.5] h. vs. 46.5 [26.6-66.4] h., resp.; p= 0.002) with a shorter duration of PT in the TSB-NICU (59 [31.8-86.2] h.) compared to the TcB-NICU (78 [37-119] h.; p< 0.001).
Conclusion(s): TcB screening with selective quantification of TSB in very preterm infants is safe when compared to daily bilirubin measurements. TcB reduced the number of TSB measurements and did not result in higher TSBmax levels across all birth weights.
Figure 1. Flow diagram of included infants in the Biliscan study.
Figure 2. Boxplot of TSBmax in different birthweight categories.