133 - 2-Year Crovalimab Paroxysmal Nocturnal Haemoglobinuria (PNH) Data for Fatigue, a Relevant Symptom in Atypical Haemolytic Uraemic Syndrome (aHUS) and PNH
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2128.133
Patty G. Leon, Genentech, San Francisco, CA, United States; Hannah Staunton, Roche Products Ltd, Welwyn Garden City, England, United Kingdom; Jennifer Stefani, F.Hoffmann-La Roche, Basel, Basel-Stadt, Switzerland
Senior Clinical Scientist Genentech San Francisco, California, United States
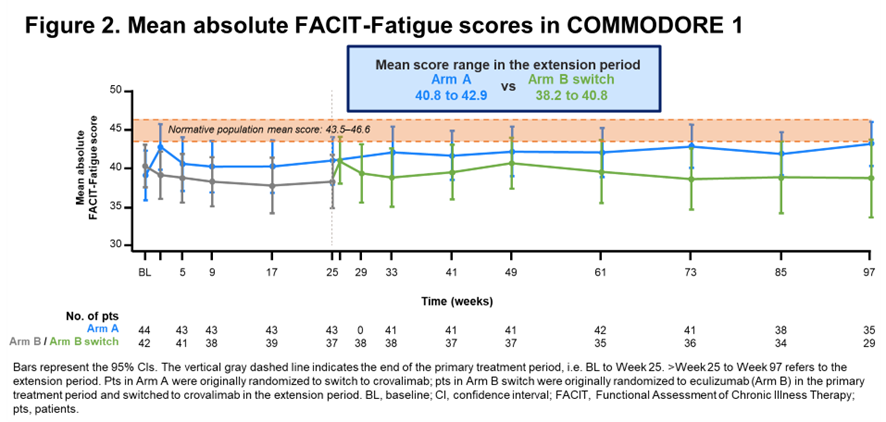
Background: aHUS is a rare, life-threatening, complement-mediated disease characterised by thrombotic microangiopathies. Established C5 inhibitors (C5is) are effective for aHUS management but typically require IV infusions. Crovalimab (crova) is a novel C5i with low-volume, subcutaneous dosing every 4 weeks, with the possibility for self-administration. Crova has also been evaluated in PNH, another complement-mediated rare blood disorder, in the global Phase III COMMODORE 2 and COMMODORE 1 trials. Objective: To evaluate fatigue in patients (pts) in COMMODORE 2 and 1. Design/Methods: COMMODORE 2 enrolled C5i-naive pts and COMMODORE 1 enrolled C5i-experienced pts with PNH. Pts were randomized to receive crova (Arm A) or eculizumab (ecu; Arm B) during the primary treatment (tx) period (baseline to Week [W] 25). After the primary tx period, pts assigned to crova continued crova (Arm A) and pts assigned to ecu (Arm B) switched to crova (Arm B switch) if continuing in the extension period (>W25). Fatigue was assessed using FACIT-Fatigue, a 13-item PRO instrument, with scoring ranging from 0-52 (higher scores indicate less fatigue). A ≥5-point score increase is a clinically meaningful improvement; the normative population mean score is 43.5-46.6. Clinical cutoff date (CCOD): Mar 12, 2024. Results: In COMMODORE 2, 129 of 135 pts randomized to crova in Arm A continued crova, and 68 of 69 pts randomized to ecu in Arm B switched to crova (Arm B switch), in the extension period. At the CCOD (median 2-year follow-up), 116 pts in Arm A and 59 in Arm B switch were receiving ongoing crova tx. At W25, Arm A pts had achieved fatigue levels similar to healthy people without PNH. Mean absolute FACIT-Fatigue scores were maintained from >W25 to 97 (Fig 1). In COMMODORE 1, all 44 pts randomized to crova in Arm A continued crova and 40 of 42 randomized to ecu in Arm B switched to crova (Arm B switch), in the extension period. At the CCOD, 42 pts in Arm A and 32 in Arm B switch were receiving ongoing crova tx. Mean absolute FACIT-Fatigue scores remained stable from >W25 to 97 (Fig 2).
Conclusion(s): In COMMODORE 2, improvements in pt-reported fatigue levels with crova in the primary tx period were maintained over a 2-year median follow-up. In COMMODORE 1, fatigue levels were stable over this same time frame. These data indicate the long-term benefit that can be achieved with crova. The COMMUTE-a (NCT04861259) and COMMUTE-p (NCT04958265) global, Phase III, single-arm trials evaluating crova in aHUS are ongoing, and include assessment of fatigue, given its importance in this population.
Figure 1. Mean absolute FACIT-Fatigue scores in COMMODORE 2
Figure 2. Mean absolute FACIT-Fatigue scores in COMMODORE 1


.png)