Session: Neonatal Hematology & Transfusion Medicine 1
161 - Patterns of transfusion and coagulation testing in early diagnosis of necrotizing enterocolitis (NEC)
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2155.161
Kirtikumar Upadhyay, University of Washington School of Medicine, SEATTLE, WA, United States; Tiffany Stanley, University of Washington School of Medicine, Seattle, WA, United States; Mehek Narmeen, Dr Ruth Pfau Civil Hospital Karachi, Baltimore, MD, United States; Aiman Tariq, University of Illinois College of Medicine- Peoria, Peoria, IL, United States; Agnes S. Chao, University of Washington School of Medicine, Seattle, WA, United States; Rida Hasan, University of Washington, Seat, WA, United States
Professor University of Washington School of Medicine SEATTLE, Washington, United States
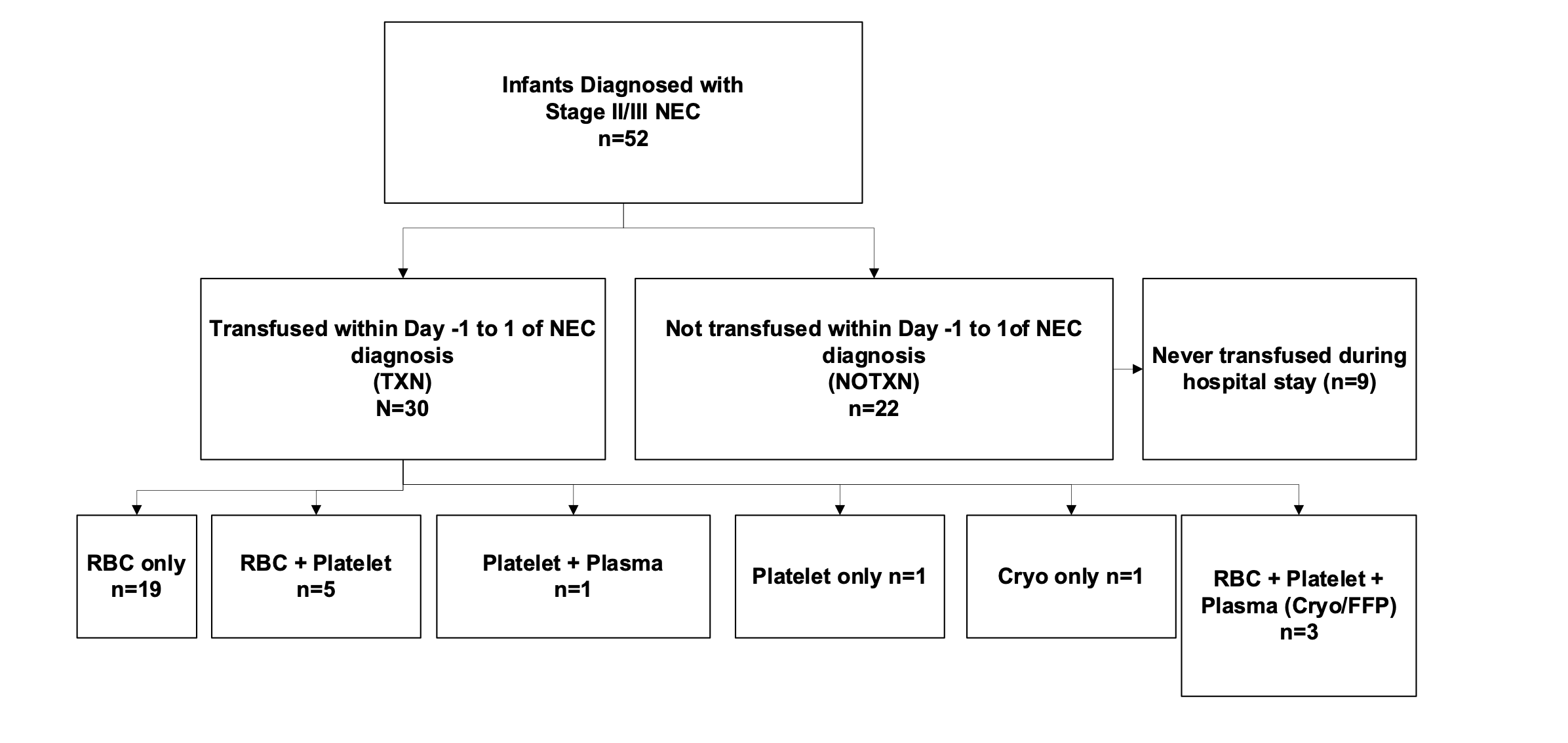
Background: Necrotizing enterocolitis (NEC) may cause bleeding and coagulopathy, but factors predicting early transfusion needs and optimal practices for coagulation testing and transfusion thresholds remain unclear. Objective: To compare characteristics, lab testing, and transfusion practices in neonates with NEC who received a transfusion from one day before to one day after diagnosis. Design/Methods: This single-center retrospective study included neonates with stage II/III NEC admitted to a level IV NICU from February 2018 to August 2024. Statistical analyses used t-tests, Mann-Whitney U tests, and Chi-square tests (OR, CI). Results: Fifty-two infants were diagnosed with Stage II/III NEC; 30 received a transfusion from Day -1 to Day +1 (TXN group), and 22 did not (NOTXN group). Red blood cells (RBCs) were the most common product transfused (90%) (Figure 1). Nineteen of 30 (63%) received only RBCs, while 11 of 30 (37%) also received platelets, fresh frozen plasma (FFP), or cryoprecipitate, alone or in combination. Infants with birthweight < 1000 g, Stage III NEC, or antenatal steroid exposure were more likely to receive transfusions (OR 4.5, 5.3, and 6.5, respectively) (Table 1).
Lab data were available for 45 of 52 infants (29 TXN, 16 NOTXN). Hemoglobin, hematocrit, and platelet counts did not differ between groups (Table 2). Coagulation studies were obtained in 11 of 52 (21%) infants, more often in those with Stage III NEC (OR 8.1, p = 0.03). Seven of 11 (64%) tested infants were coagulopathic; six received plasma transfusions, and one died before transfusion. Infants receiving FFP had higher INR values (2.1 vs 1.3, p = 0.04), and all with INR > 2 received FFP, while fibrinogen levels did not differ between groups.
Conclusion(s): NEC stage and birthweight may help predict which neonates require transfusions early in the disease. Coagulation testing is not standard practice and was performed in fewer than 20% of cases, despite a high incidence of coagulopathy. All infants with INR > 2 received FFP, but transfusion practices for RBCs, platelets, and cryoprecipitate varied widely. Further studies are needed to define optimal coagulation testing and transfusion strategies during early NEC.
Figure 1: Flowchart of transfusion practices in neonates with NEC from one day before to one day after diagnosis
Table 1: Baseline Characteristics
Table 2: Laboratory testing and transfusion requirements

.png)
.png)
