100 - Provider and Staff Perceptions about Care Delivery, Discrimination, and Medical Mistrust in Clinics with Varying Levels of Segregation of Care by Insurance and Race/ethnicity
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2095.100
Nita Vangeepuram, Icahn School of Medicine at Mount Sinai, New York, NY, United States; Radhi Yagnik, Icahn School of Medicine at Mount Sinai, Somerset, NJ, United States; Lauren Gordon, Icahn School of Medicine at Mount Sinai, New York, NY, United States; Lobsang Palmo, Icahn School of Medicine at Mount Sinai, Crystal, MN, United States; Carol Horowitz, Icahn School of Medicine at Mount Sinai, New York, NY, United States; Lynne D.. Richardson, Icahn School of Medicine at Mount Sinai, New York, NY, United States; Nina Bickell, Icahn School of Medicine at Mount Sinai, New York, NY, United States
Associate Professor Icahn School of Medicine at Mount Sinai New York, New York, United States
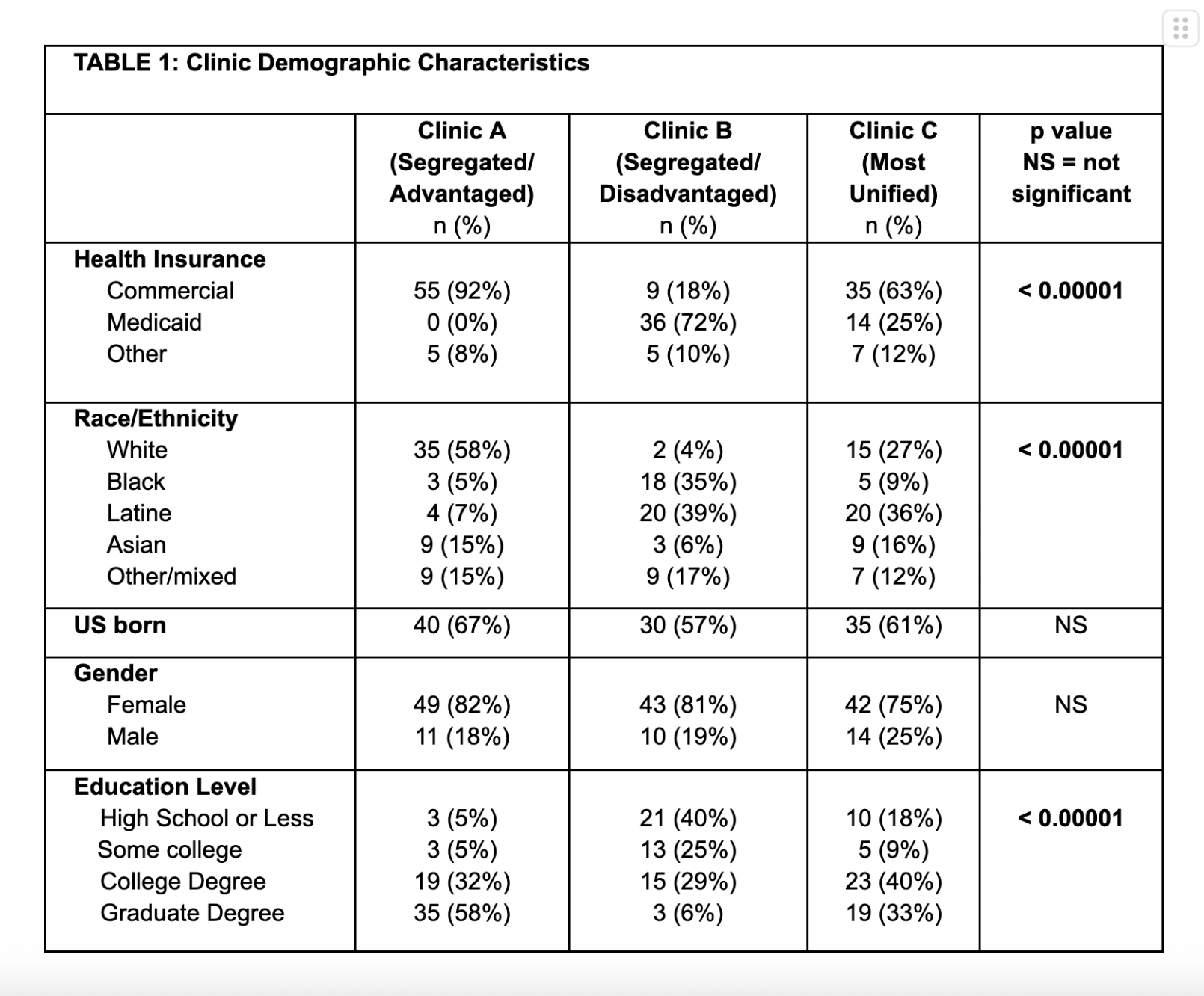
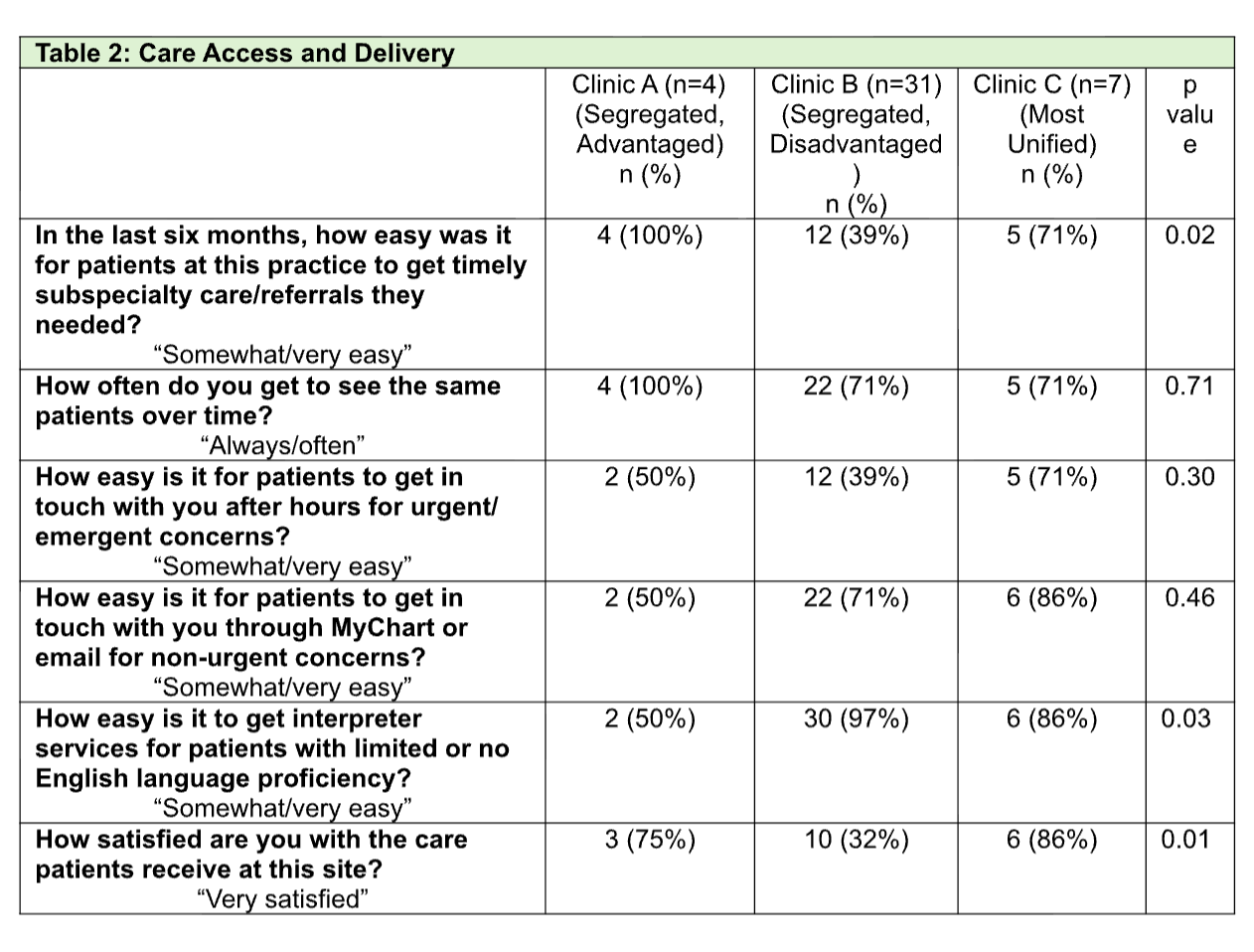
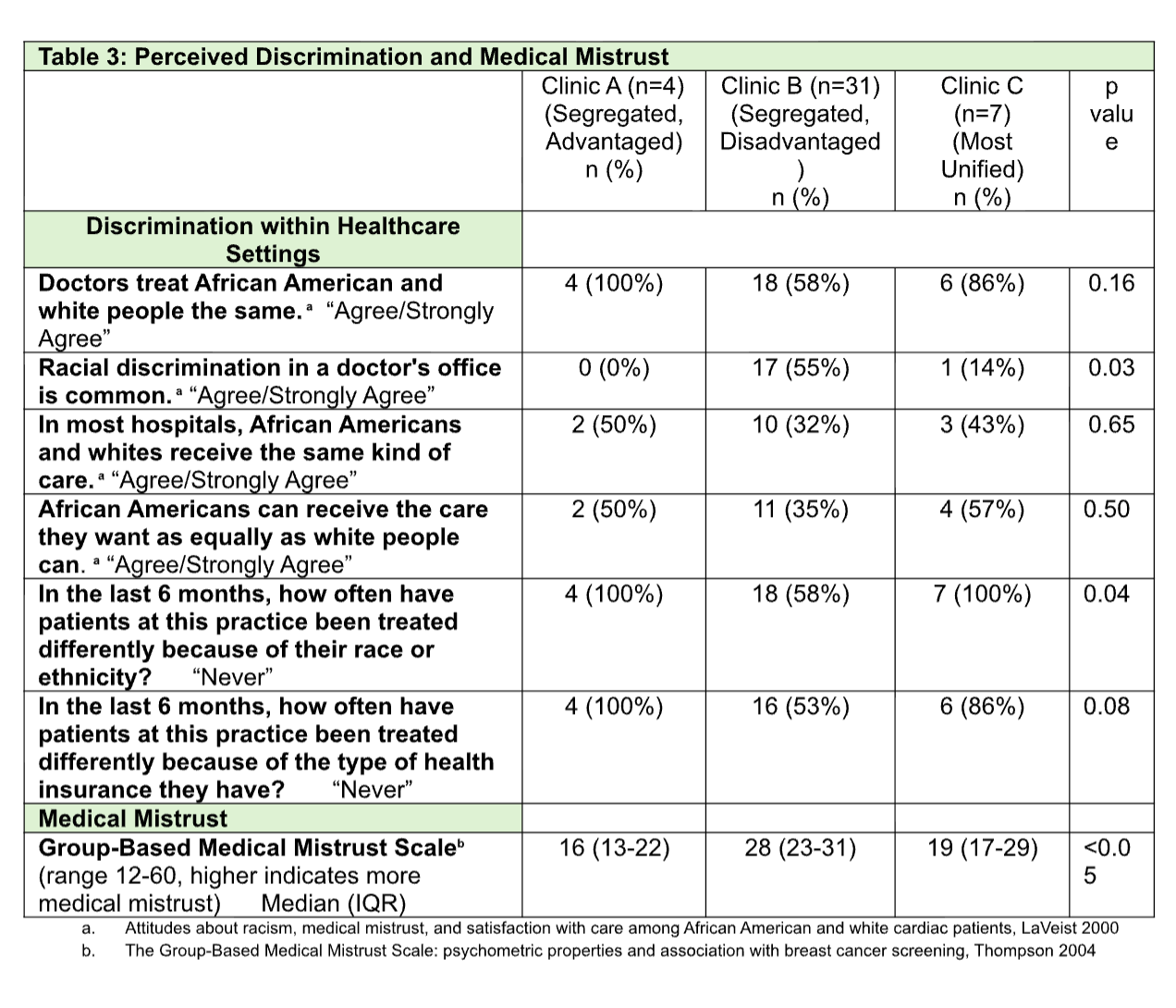
Background: Structural racism persists in healthcare and may affect perceptions about care delivery, discrimination, and medical mistrust among providers and staff in clinics with varying levels of segregation of care by insurance and race/ethnicity. Objective: To identify ambulatory practices with varying levels of segregation by insurance and race/ethnicity and examine perceptions among providers and staff on care access and delivery, level of satisfaction with care, discrimination in healthcare settings, and medical mistrust in more and less segregated pediatric practices. Design/Methods: We identified pediatric clinics from a large urban health system with varying levels of segregation based on composite scores calculated from the distribution of patients by insurance and race/ethnicity. We identified 3 clinics: most segregated and advantaged (Clinic A); most segregated and disadvantaged (Clinic B); and most unified (Clinic C). We surveyed 76% of providers and staff across clinics and examined differences in outcomes of interest using Fisher Exact and Kruskal Wallis tests. Results: Clinics A, B, and C varied by race/ethnicity (58%, 4%, and 27% White, respectively, p< 0.00001) and Medicaid insurance (0%, 72%, and 25% respectively, p< 0.00001). Table 1 includes additional clinic demographic characteristics. Survey respondents (n=42) included attending physicians (24%), nurses (17%), medical assistants (17%), social workers (17%), administrative staff (19%) and other (7%). Respondents self-described as White (26%), Black (24%), Hispanic (43%) and mixed/other race (7%). Table 2 includes respondents' perceptions about care access and delivery with significant differences across clinics in perceived ease in getting timely subspecialty care and level of satisfaction with care received (lower in clinic B) and perceived ease in getting interpreter services (lower in clinic A). Table 3 includes respondents' perceptions about discrimination in healthcare settings and medical mistrust. Respondents from clinic B were more likely to report that racial discrimination in a doctor's office is common, that patients at their practice had been treated differently because of their race or ethnicity, and had higher medical mistrust.
Conclusion(s): Overall, providers and staff from the most segregated and disadvantaged pediatric clinic were more likely to report challenges with care access, lower satisfaction with care delivered, and more perceived discrimination and medical mistrust. Future research will examine whether these differences are associated with differences in quality metrics.
TABLE 1: Clinic Demographic Characteristics
TABLE 2: Care Access and Delivery
Table 3: Perceived Discrimination and Medical Mistrust

 photo")