TOP 33 - Optimizing Diuretic Management in Extremely Preterm Infants with Evolving Chronic Lung Disease Using Point-of-Care Ultrasound (POCUS)
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3762.TOP 33
Sheryar Siddiqui, UC Irvine/CHOC, Orange, CA, United States; Ayan Rajgarhia, CHOC Children's Hospital of Orange County, Orange, CA, United States; Michel Mikhael, CHOC Children's Hospital of Orange County, Orange, CA, United States
Fellow Physician Rady Children's Health | UC Irvine Orange, California, United States
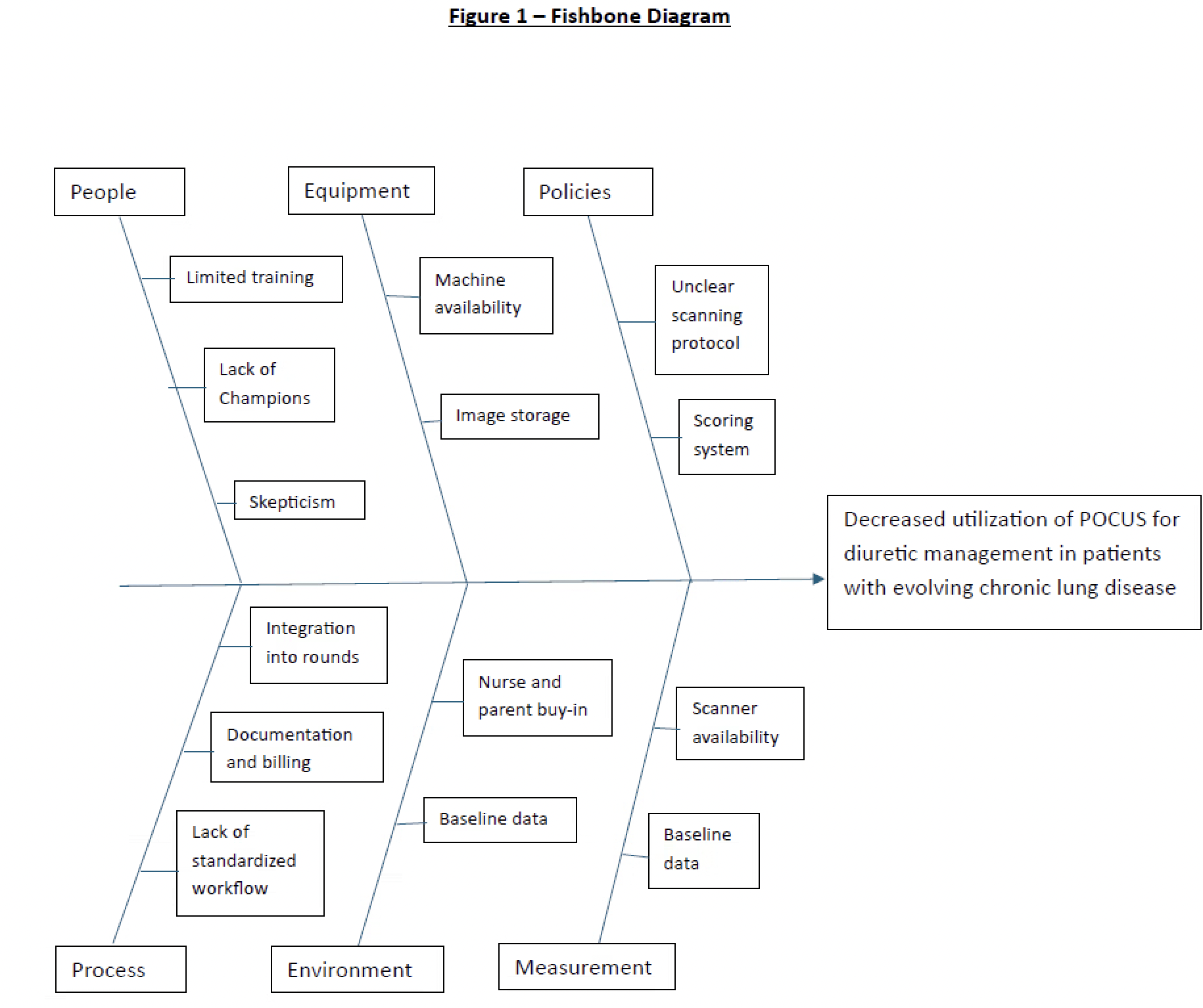
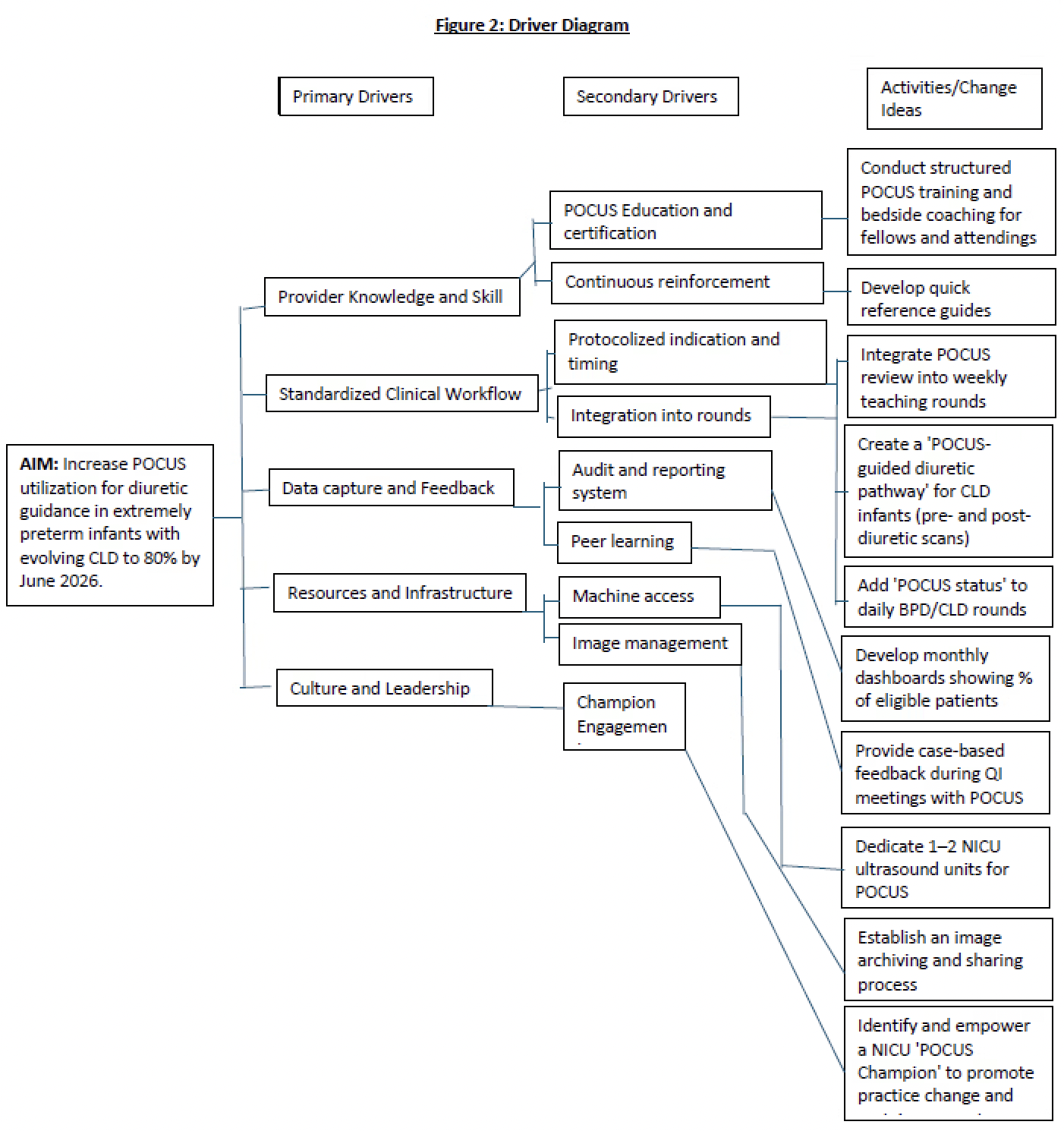
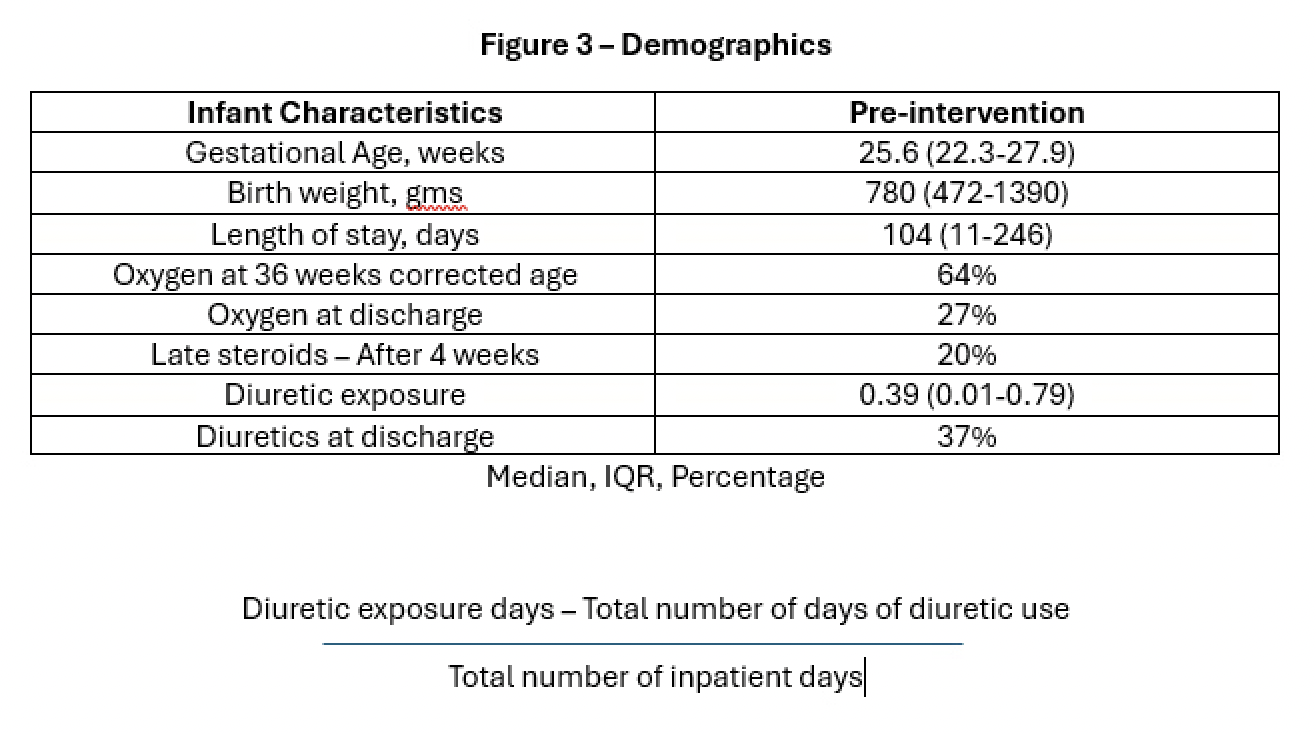
Background: Although widely used in the NICU for Bronchopulmonary Dysplasia (BPD), diuretics remain controversial. While they offer short-term benefits, no RCTs have shown effects on hospital stay, oxygen or mechanical ventilation (MV) duration, or BPD incidence. Their use remains variable with no proven long-term advantage. Advances in lung ultrasound (LUS) and point-of-care ultrasound (POCUS) enable more sensitive detection of pulmonary edema. Using POCUS to guide diuretic therapy in evolving chronic lung disease (CLD) could reduce unnecessary exposure, optimize timing and dosing, minimize renal/electrolyte complications, and promote individualized, evidence-based care. Objective: Implement a QI initiative to increase the use of POCUS to guide diuretic therapy in preterm infants with CLD, with the goal of optimizing their use in this population. Design/Methods: We designed a QI project with a SMART Aim to increase POCUS use for diuretic guidance in infants < 28 weeks gestation and >2 weeks old with evolving CLD. A fishbone diagram (Figure 1) identified causes for low POCUS utilization and informed our driver diagram (Figure 2). Outcome measures: percentage of eligible infants with POCUS-guided diuretic use, number diagnosed with BPD, diuretic exposure (diuretics therapy days/length of stay), steroid rescue after 34 weeks corrected age, and discharge on diuretics. Process measures: protocol compliance, number of trained/credentialed providers, weekly POCUS evaluations, and EHR documentation of findings. Balancing measures: delay in diuretic initiation, unplanned fluid/electrolyte issues, and probe-related skin breakdown. Four Plan-Do-Study-Act (PDSA) cycles targeted training and awareness, protocol development, pilot data collection, integration/feedback, and sustainability were developed with the first PDSA already being implemented. Ongoing PDSA cycles will continue over the next 3 months aimed at increasing POCUS utilization for diuretic management in evolving CLD to 80% along with data collection and monitoring of our outcome measures.

 Credit")