721 - Variation in Emergency Department Management of Pediatric Palatal and Posterior Oropharyngeal Trauma
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3698.721
Tyler W. Ellis, Children's Hospitals and Clinics of Minnesota, Minneapolis, MN, United States; Janeen Manuel, Children's Hospitals and Clinics of Minnesota, Minneapolis, MN, United States; Henry W. Ortega, Children’s Minnesota, Minneapolis, MN, United States
Fellow Children's Hospitals and Clinics of Minnesota Minneapolis, Minnesota, United States
Background: While penetrating palatal and oropharyngeal trauma is rare, significant complications can occur, including cerebrovascular injury and death. Young children are at particular risk due to their propensity to fall with objects in their mouths. Prior research has shown variable management of these injuries. Objective: To explore variables associated with the prescription of antibiotics, imaging orders, and disposition in the management of palatal and posterior oropharyngeal trauma in children presenting to the ED. Design/Methods: We performed a retrospective study of pediatric patients at a single institution between 2016-2024. Primary outcomes included antibiotic prescription, imaging orders, and disposition. Univariate associations between each outcome and variables of interest were assessed using chi-square, Fisher's exact tests, or linear-by-linear (LBL) association tests (ordinal variables), with statistically significant (P < 0.10) variables entered into subsequent multivariable logistic regressions. Variables of interest included injury location, laterality of injury, injury size, mechanism of injury, and patient age. Results: Data from 178 patients were collected, with 2 cases excluded for polytrauma. Common objects of injury were drinking straws, toothbrushes, pens/pencils, and sticks. The most common imaging modality was lateral neck x-ray (16.5%), followed by neck CTA (11.9%). Antibiotics were prescribed in 31.3% of patients, most commonly Augmentin and Unasyn. Forty-three patients (24.4%) were admitted. Five patients (2.8%) were transferred from the ED to OR. Four patients (2.3%) returned to the ED after initial evaluation, with three requiring admission (positive blood culture, pain control, and abscess). No patient experienced cerebrovascular injury or death (Table 1).
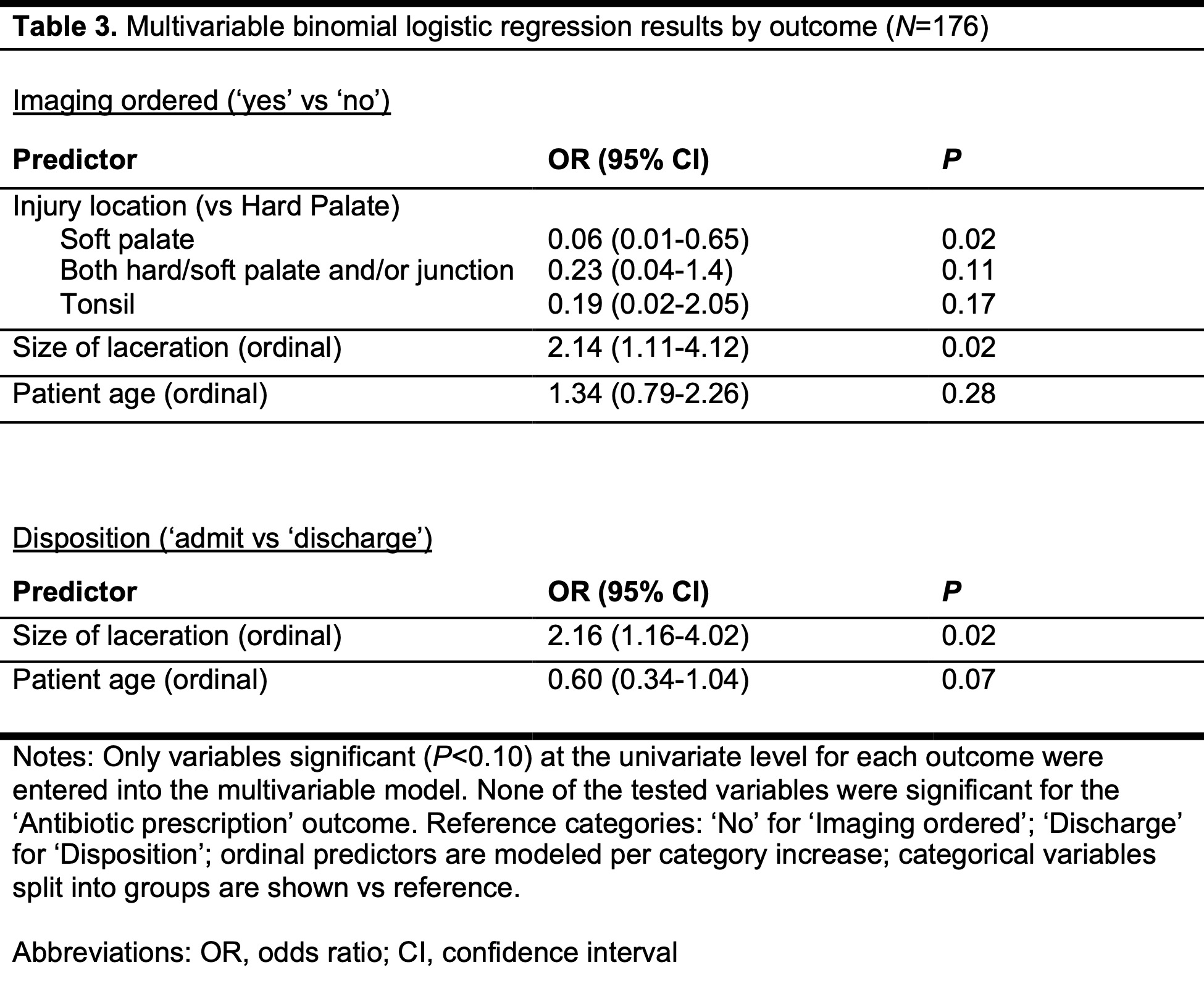
At the univariate level, no variables were associated with antibiotic prescription; three were associated with imaging orders, and two with disposition (Table 2). Table 3 shows the results of the multivariable logistic regressions. For imaging orders, soft palate injuries were more likely to receive imaging than hard palate (P=0.02). Patients with larger lacerations were more likely to receive imaging (P=0.02), while age was not significant. For disposition, larger lacerations were more likely to be admitted (P=0.02), and younger patients trended toward higher odds of admission (P=0.07).
Conclusion(s): This study finds that wide practice variation exists in the management of these traumatic injuries. Further studies to aid in standardization of care are needed.
Table 1. Characteristics of Study Participants
Table 2. Univariate analysis of categorical predicators by outcome variable
Table 3. Multivariable binomial logistic regression results by outcome

.jpg)
.jpg)