288 - Quality Improvement and Equity: A Multisite Study of Disparities in Pediatric Mental Health Interventions
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3277.288
Shilpa J.. Patel, Children's National Hospital, Bethesda, MD, United States; Katharine Clouser, Hackensack Meridian School of Medicine, Hackensack, NJ, United States; Ellen Kerns, University of Nebraska Medical Center, Omaha, NE, United States; Makayla Schissel, University of Nebraska College of Medicine, Omaha, NE, United States; Jennifer Monti, American Academy of Pediatrics, Itasca, IL, United States; Carla Allan, Phoenix Children's Hospital, Phoenix, AZ, United States; Hendi Berrios, Duke University Hospital, Durham, NC, United States; Amanda Burnside, Northwestern University The Feinberg School of Medicine, Chicago, IL, United States; David Chaulk, University of Calgary, Calgary, AB, Canada; Andrea Dean, Baylor College of Medicine, Houston, TX, United States; Stephanie Doupnik, Vanderbilt University School of Medicine, Nashville, TN, United States; Melissa M.. Doyle, Bernard Millie Duker Childrens Hospital, Albany, NY, United States; Jeremy Esposito, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Benjamin Fogel, Pennsylvania State University College of Medicine, Hershey, PA, United States; Kyle P. Johnson, Oregon Health & Science University, Portland, OR, United States; Brett Palama, University of Chicago, Chicacgo, IL, United States; Paul Mullan, Children's Hospital of The King's Daughters, Norfolk, VA, United States; Steven C. Rogers, University of Connecticut School of Medicine, Hartford, CT, United States; Sara Lee, Akron Children's Hospital, Akron, OH, United States; Kendall Arslanian, American Academy of Pediatrics, Chicago, IL, United States; Sloane Magee, The American Academy of Pediatrics, Aurora, IL, United States; Brittany Jennings, American Academy of Pediatrics, Itasca, IL, United States; Michelle Noelck, Doernbecher Children's Hospital at Oregon Health & Science University, Portland, OR, United States; Olivia Ostrow, The Hospital for Sick Children, Toronto, ON, Canada
Associate Professor of Pediatrics and Emergency Medicine Children's National Hospital Bethesda, Maryland, United States
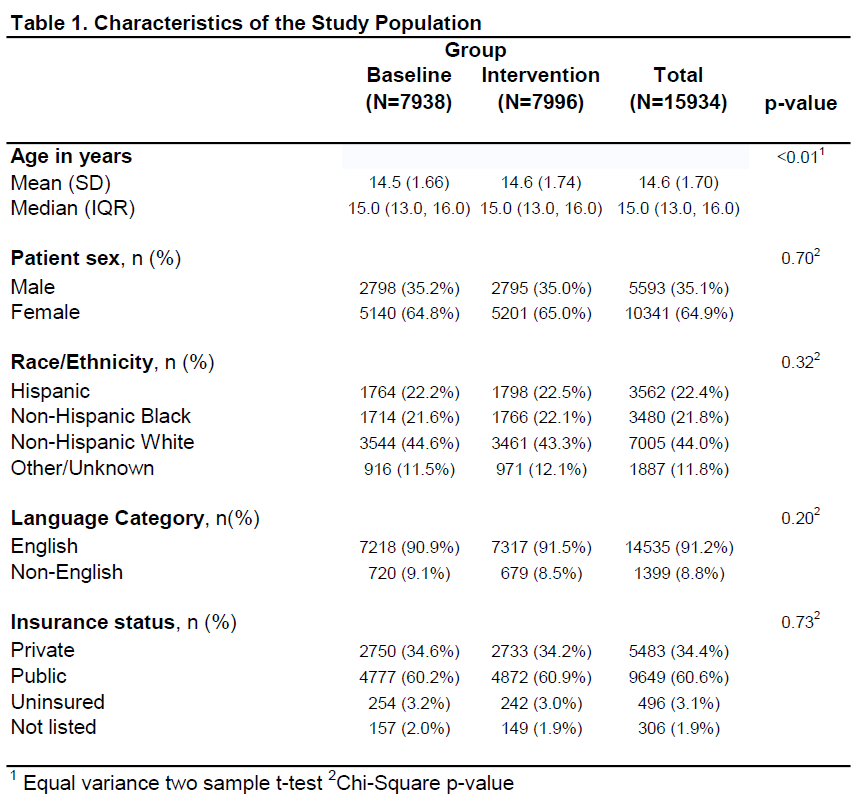
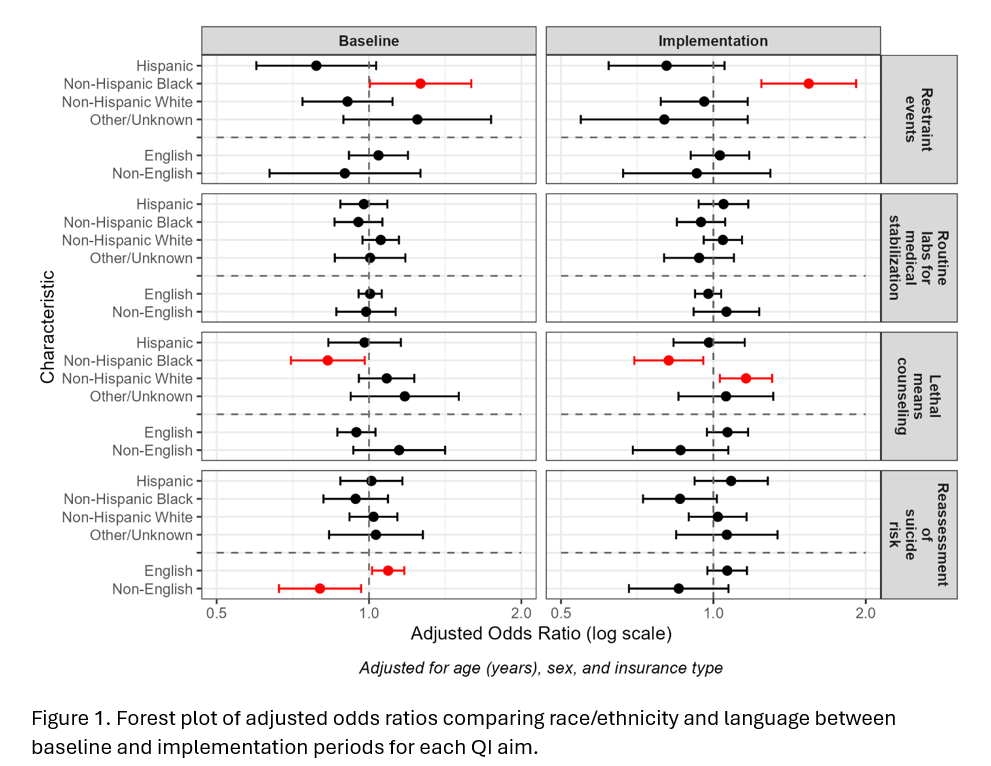
Background: Racial, ethnic, and language disparities are well described in hospital-based mental health care for youth in the US. The impact of standardizing care through quality improvement (QI) on these disparities remains understudied. The American Academy of Pediatrics (AAP) Pediatric Acute and Critical Care (PACC) Quality Network conducted a multicenter QI collaborative project to improve care for children ages 12-17 presenting to the emergency department or hospital for an acute mental health concern. Objective: To compare disparities related to race/ethnicity and language in the four aims of the QI collaborative: 1) reducing physical restraint events, 2) reducing routine labs for medical stabilization, 3) increasing lethal means counseling and 4) increasing reassessment of suicide risk. Design/Methods: We conducted a mixed-effect logistic regression analysis, adjusting for age(years), sex, insurance type and hospital setting to evaluate disparities in each outcome by race/ethnicity (Hispanic, non-Hispanic Black, non-Hispanic White, Other/Unknown) and language (English, non-English) within both the baseline and intervention periods. All groups were compared to the total population. Hospitals entering at least 75% of data for both implementation and baseline periods were included. Results: 37 of 54 participating hospitals were included (Table 1). Racial/ethnic disparities were found in restraint events at baseline (adjusted odds ratio (aOR) 1.264, 95% CI 1.004, 1.593) and worsened slightly during implementation (aOR 1.543, 95% CI 1.233, 1.914). Similarly, disparities were identified for lethal means counseling in the baseline (aOR 0.829, 95% CI 0.701, 0.981) and persisted through implementation (aOR 0.816, 95% CI 0.698, 0.955). Language-related disparities in reassessment of suicide risk improved from baseline (English: aOR 1.091, 95% CI 1.014, 1.174; non-English: aOR 0.800, 95% CI 0.664, 0.965) with no significant differences noted during implementation (English: aOR 1.065, 95% CI 0.973, 1.165; non-English: aOR 0.854, 95% CI 0.681, 1.071). No disparities were detected in the use of routine labs for medical stabilization (Figure 1).
Conclusion(s): Consistent with prior literature, NH Black youth had higher odds of restraint events as compared to all other races combined. We also found lower rates of lethal means counseling among NH Black youth. Our efforts to standardize care may have alleviated disparities in the reassessment of suicide risk. Equity centered strategies embedded in QI are needed to improve disparities in pediatric mental health care.
Table 1. Characteristics of the Study Population
Figure 1. Forest plot of adjusted odds ratios comparing race/ethnicity and language between baseline and implementation periods for each quality improvement aim.

 photo")