552 - Limited Prognostic Value in Fetal Heart Rate Tracing Characteristics in Preterm Deliveries <32 Weeks Gestation
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3533.552
Ha Tran, Sidney Kimmel Medical College at Thomas Jefferson University, PHILADELPHIA, PA, United States; Lauren C. London, Christiana Care Health System, Newark, DE, United States; Lydia Deaton, ChristianaCare, Newark, DE, United States; Suneet Chauhan, ChristianaCare Hospital, Newark, DE, United States; Vasiliki Anemikos, ChristianaCare, Wilmington, DE, United States; Keshab Subedi, Christiana Care Health System, Wilmington, DE, United States; Fabrizio Zullo, Sapienza University of Rome, Rome, Lazio, Italy; Cassidy A. O'Sullivan, Christiana Care Health Services, Wilmington, DE, United States; Amanda J. Jones, Christiana Care Health System, Wilmington, DE, United States; Rachel Wiley, University of California, San Diego, San Diego, CA, United States; Matthew K. Hoffman, CHRISTIANA CARE, Newark, DE, United States; Anthony Sciscione, Christiana care, Newark, DE, United States; Kelley Kovatis, ChristianaCare, Newark, DE, United States
NICU Fellow Sidney Kimmel Medical College at Thomas Jefferson University PHILADELPHIA, Pennsylvania, United States
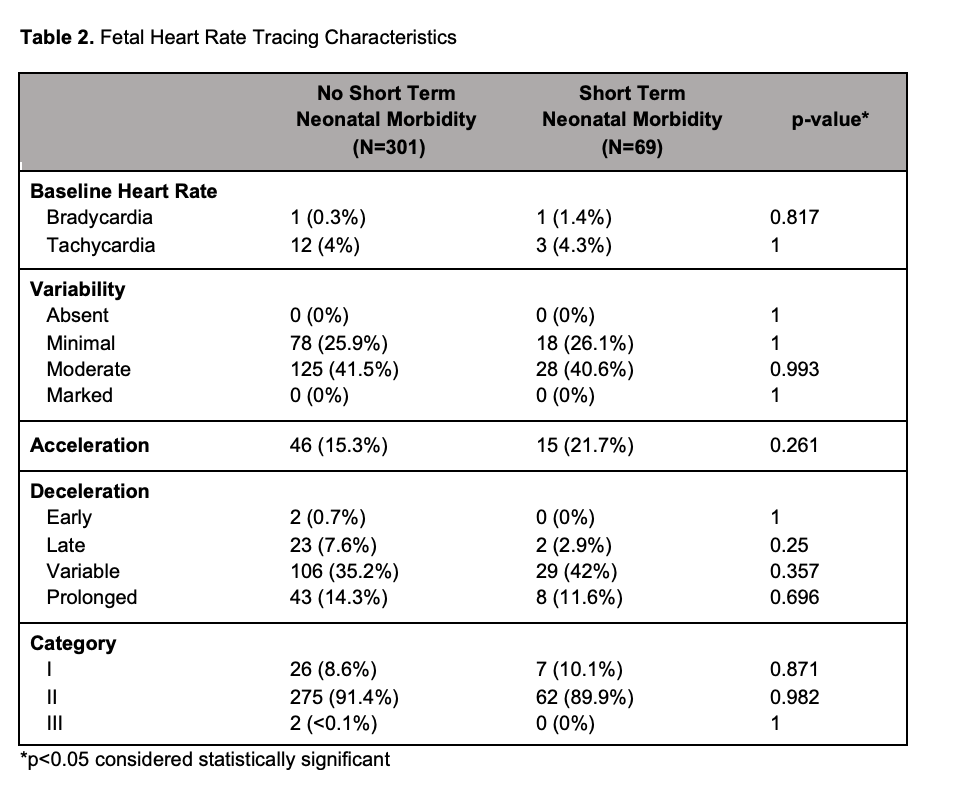
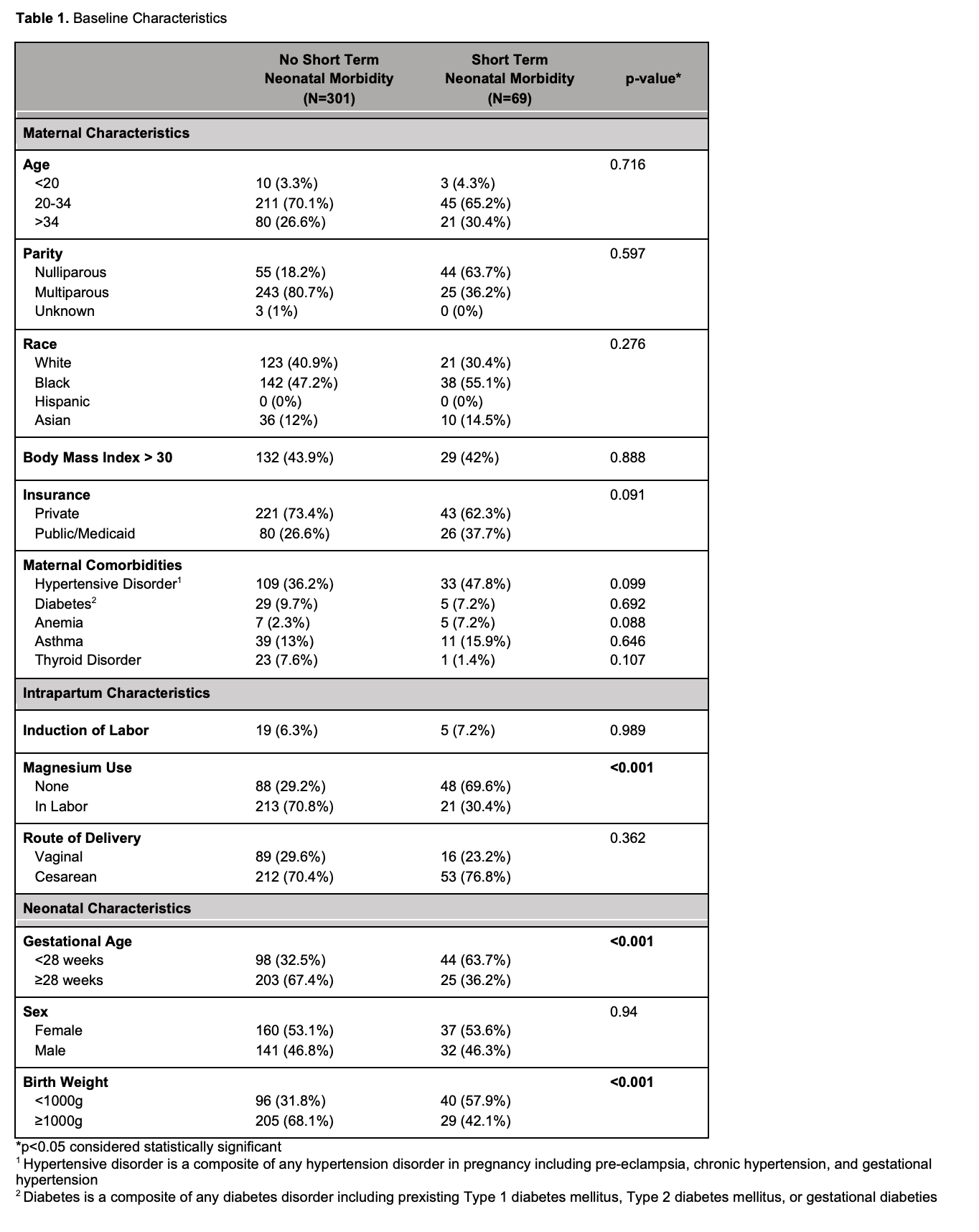
Background: Fetal heart rate tracing (FHRT) is used to assess the physiologic response to changes in fetal oxygenation during labor. The American College of Obstetricians and Gynecologists' three-tier FHRT classification provides a framework for evaluating fetal tolerance during labor, categorizing tracings as reassuring (I), indeterminate (II), or non-reassuring (III). Despite longstanding reliance on FHRT in term deliveries, there remains a critical gap in understanding the prognostic significance of FHRT among preterm deliveries. Filling this gap has the potential to directly inform clinical guidelines, reduce unnecessary interventions, and improve patient outcomes. Objective: To evaluate the prognostic value of the FHRT in preterm deliveries by examining its association with adverse outcomes. Design/Methods: This retrospective cohort study included non-anomalous singleton deliveries between 22.0-31.6 weeks gestation from 2021-2024 at a tertiary referral hospital. A physician, blinded to neonatal outcomes, reviewed FHRT tracings two hours preceding delivery. The primary outcome was short-term neonatal morbidity (STNM), defined as 5-minute APGAR ≤3, severe metabolic acidosis, or advanced delivery room resuscitation (i.e. endotracheal intubation, chest compressions, and/or administration of epinephrine). Logistic regression was used to examine associations between FHRT and neonatal outcomes with multivariable models adjusted for neonatal and maternal covariates. Results: Among 25,706 deliveries, 614 (2%) occurred at 22.0-31.6 weeks with 370 patients meeting the inclusion criteria. STNM occurred in 19% of patients, with 7 neonatal deaths within 48 hours of birth (Table 1). Magnesium sulfate use was lower in the STNM group (30.4% vs 70.8%, p< 0.05). When stratified by gestational age at delivery ( < 26, 26-27.6, and ≥28 weeks), Category I tracings were observed in 11%, 8%, and 8% of cases, while Category II tracings occurred in 66%, 64%, and 49%, respectively (Figure 1). Among infants with documented delivery indications, 44% were delivered for non-reassuring FHRT. Neither the three-tier FHRT classification nor individual FHRT characteristics were predictive of STNM (Table 2). The only significant predictor of STNM was gestational age (aOR 0.72 per week, 95% CI 0.59-0.94, p< 0.01) and birth weight (OR 2.95, 95% CI 1.73-5.02, p< 0.01).
Conclusion(s): These results indicate that FHRT offers limited prognostic value for preterm infants and should not be used as an indication for delivery. The study emphasizes the need for alternative strategies to guide clinical decision-making.
Table 1. Baseline Characteristics
Figure 1. Distribution of Fetal Heart Rate Tracing Categories Across Gestational Age

 photo")
.png)