724 - Factors associated with prolonged hospitalization and adverse outcomes in injured children in a regional health system
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3700.724
Liz Lendrum, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; David Schnadower, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Meera Kotagal, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Paria M. Wilson, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Holly Hanson, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Wendy Pomerantz, Cincinnati Children's Hospital Medical Center, BLUE ASH, OH, United States; Allan M. Joseph, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Yin zhang, Cincinnati Children's Hospital Medical Center, West Chester, OH, United States; Kenneth Michelson, Lurie Children's Hospital, Chicago, IL, United States
Clinical Fellow Cincinnati Children's Hospital Medical Center Cincinnati, Ohio, United States
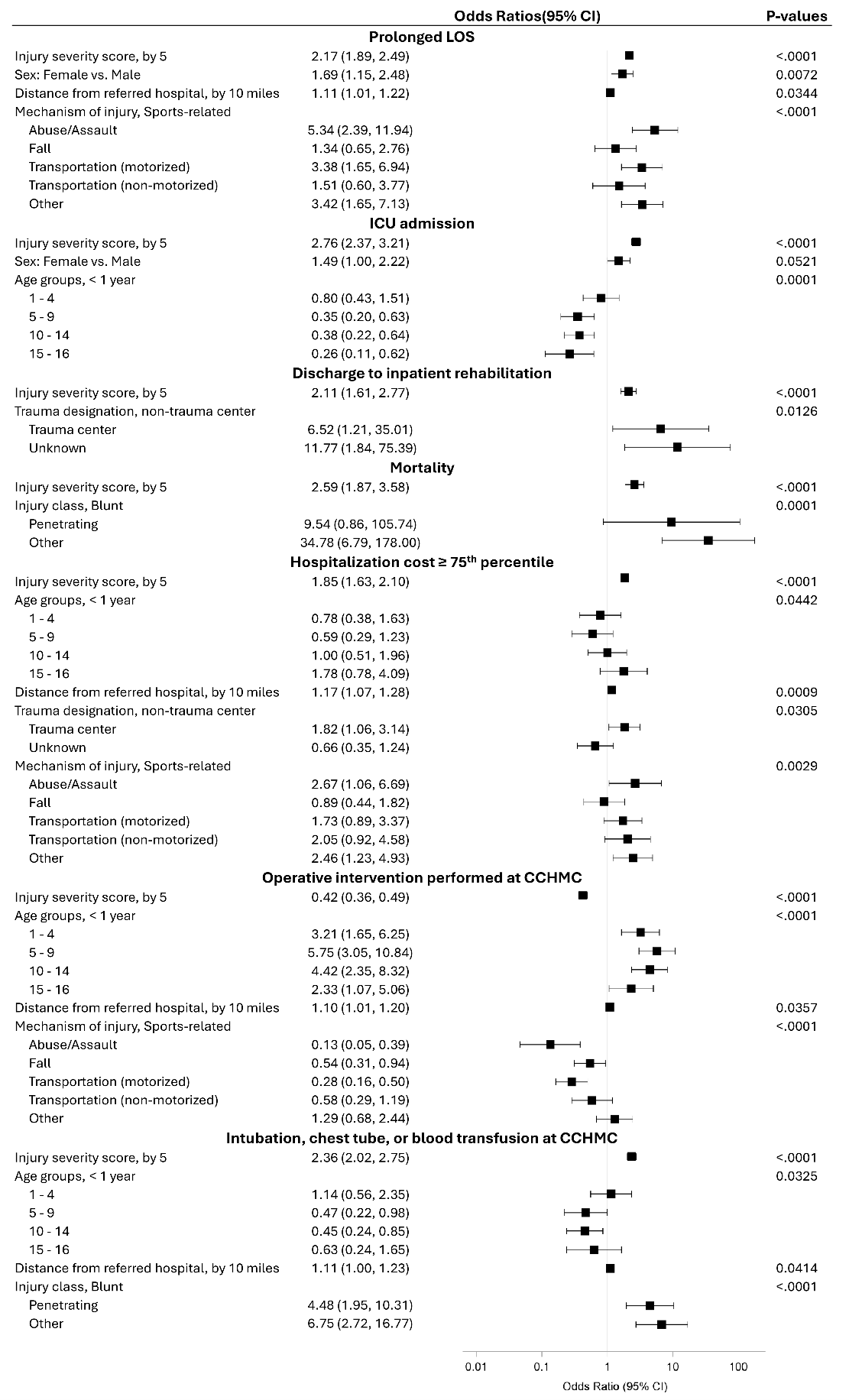
Background: Improving pediatric trauma outcomes requires timely access to specialized care. In the US, most injured children are not initially evaluated at pediatric trauma centers (PTC). Identification of visit- and hospital-level factors associated with adverse outcomes is needed for system-level improvements. Objective: (1) Evaluate the association of transfer status with prolonged hospital length of stay (LOS) and (2) Identify visit- and hospital-level factors associated with adverse outcomes in children transferred to a regional level one PTC. Design/Methods: Retrospective cohort study of injured children < 16 years of age admitted to a regional Level I PTC from 2018-2024. Exposure variable was transfer status (direct vs interfacility). Primary outcome was prolonged LOS, defined as highest LOS quartile. Secondary outcomes included need for intensive care unit (ICU), inpatient rehabilitation, surgery, critical intervention (intubation, chest tube, transfusion), high cost (top quartile), and death. We excluded children with low-acuity short-stay admissions (defined as LOS < 36 hours without ICU care, surgery, or death), burn injuries (as our institution is not a burn center), and prior trauma admissions within 30 days. For objective 1, we used generalized linear mixed models, controlling for injury severity score (ISS) and other confounders. For objective 2, we used LASSO to identify the most relevant predictors. Results: Of 2,427 in our cohort, 981 (40.4%) were interfacility transfers. Unadjusted analyses showed transferred patients had lower rates of prolonged LOS, ICU admission, inpatient rehab discharge, and high-cost hospitalization. After adjustment for severity and other confounders, only need for inpatient rehabilitation (OR 0.50, 95% CI 0.28-0.92) and high cost (OR 0.68, 95% CI 0.53-0.85) remained less common in transferred patients. (Table 1) Among transfers, higher ISS and greater distance from the referring hospital predicted prolonged LOS, ICU admission, high-cost hospitalization, and critical interventions; trauma center referrals were associated with inpatient rehabilitation. (Figure 1)
Conclusion(s): Transfer status was not associated with adverse outcomes in injured patients admitted to a level one PTC, but several visit- and hospital-level variables were associated with adverse outcomes. Future work should identify subgroups within pediatric trauma systems where targeted interventions could improve outcomes.
Table 1. Outcomes by transfer status in severely injured children
Figure 1. Predictors of adverse outcomes among transferred pediatric trauma patients

 photo")
.png)