134 - Optimizing ETT Depth and Preventing Unplanned Extubation in Neonates via
Utilizing Gestational Age Charts: A QI Interventions
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3128.134
Mahmoud Ali, West Virginia University Children's Hospital, Morgantown, WV, United States; Stephanie Marks, WVU Medicine Children's, Morgantown, WV, United States; Donna L. Householder, West Virginia University Children's Hospital, Morgantown, WV, United States; Jamie R. Rice, West Virginia University Children's Hospital, Fairmont, WV, United States; Brian Ringler, West Virginia University Children's Hospital, Morgantown, WV, United States; Bronson Herr, West Virginia University School of Medicine, Worthington, WV, United States; Autumn Kiefer, West Virginia University School of Medicine, Morgantown, WV, United States
Assistant professor of pediatrics West Virginia University Children's Hospital Morgantown, West Virginia, United States
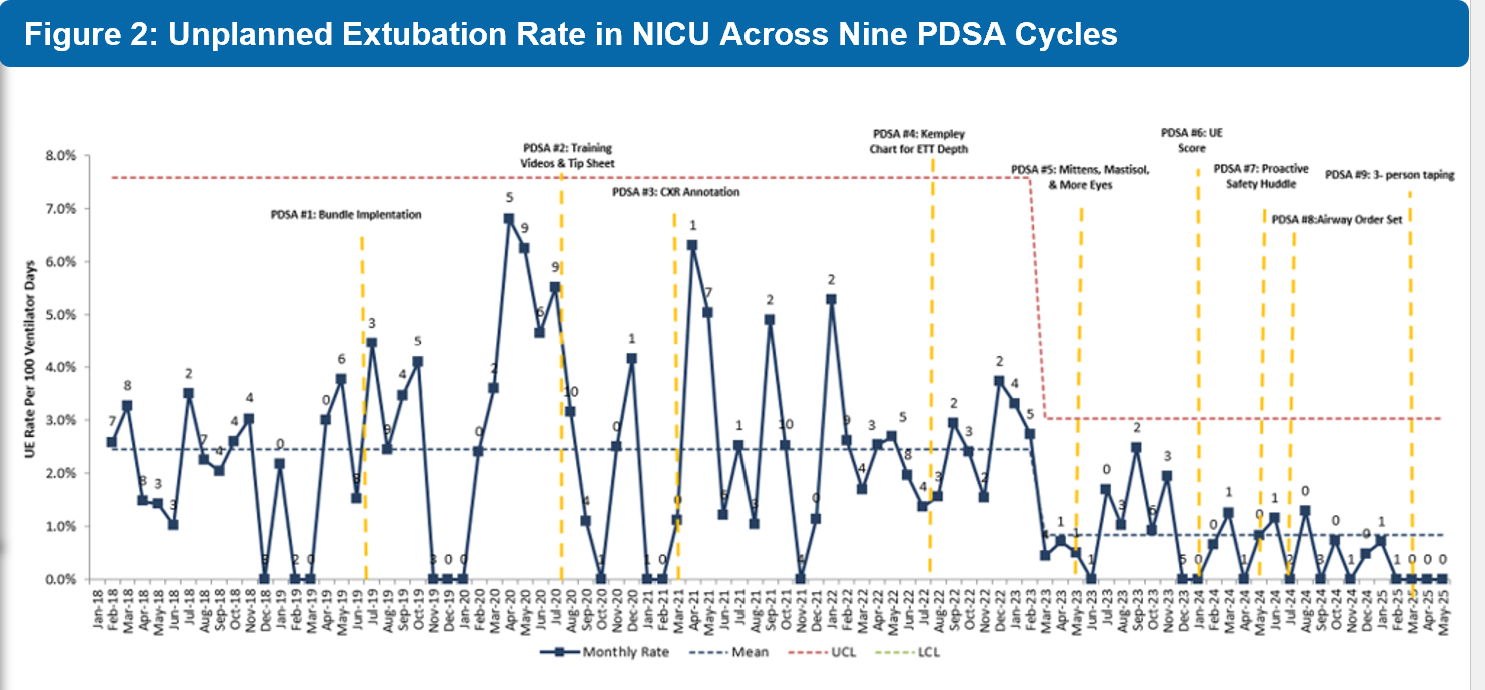
Background: Unplanned extubations (UEs) are the fourth most common adverse event in the NICU and pose serious risks, including airway trauma, infection, prolonged ventilation, bronchospasm, and cardiopulmonary compromise. Emergency reintubation further increases the risk of tracheal and pulmonary injury, intracranial pressure changes, brain hemorrhage, and bradycardia. UEs are a key quality-of-care metric. Objective: To reduce UEs by 33% in our NICU to 1.6 per 100 ventilator days over 18 months Design/Methods: We applied a standardized UE prevention bundle nationally available through the Solutions for Patient Safety (SPS) network that included the use of 2 caregivers for movement of intubated neonates and standardization of patient positioning during chest imaging. UEs significantly decreased after standardizing the prescribed ETT depth for ventilated neonates. using a gestational age-based chart adapted from the Kempley study to preemptively anticipate changes needed in the prescribed ETT depth over time. Serial Plan-Do-Study-Act (PDSA) cycles were necessary to achieve the desired outcome. Results: Sample included 48.7% females, 46.5% Caucasians, 97.3% singleton, and 1.64% SGA) infants. Between 2019 and 2024, our NICU tracked 204 unplanned extubations (UEs) over 10,176 ventilator days (2.0/100 days). Baseline UE rates in 2017-2018 were ~2.4/100 days, with little change after early interventions. In 2020, rates peaked at 3.67/100 days despite improved compliance with 2-caregiver movement. Introduction of a gestational age-based ETT depth chart in mid-2022 halved UE events. Continued improvements in compliance (≥98% in 2023) and additional quality measures-including a UE scoring tool, safety huddles, and airway order sets-drove the rate down to 0.58/100 days in 2024, a 76% reduction from peak and well below institutional targets. Overall, from 2022 to 2024, UEs decreased by 79% (49 vs. 10), with sustained compliance above national benchmarks and no rise in pneumothorax.
Conclusion(s): This QI project at WVU Children's Hospital NICU reduced unplanned extubations by 79% through standardized protocols, staff education, a gestational age-based ETT depth chart, SPS bundle adherence, improved taping, and consistent imaging. Reducing UEs enhanced neonatal safety.
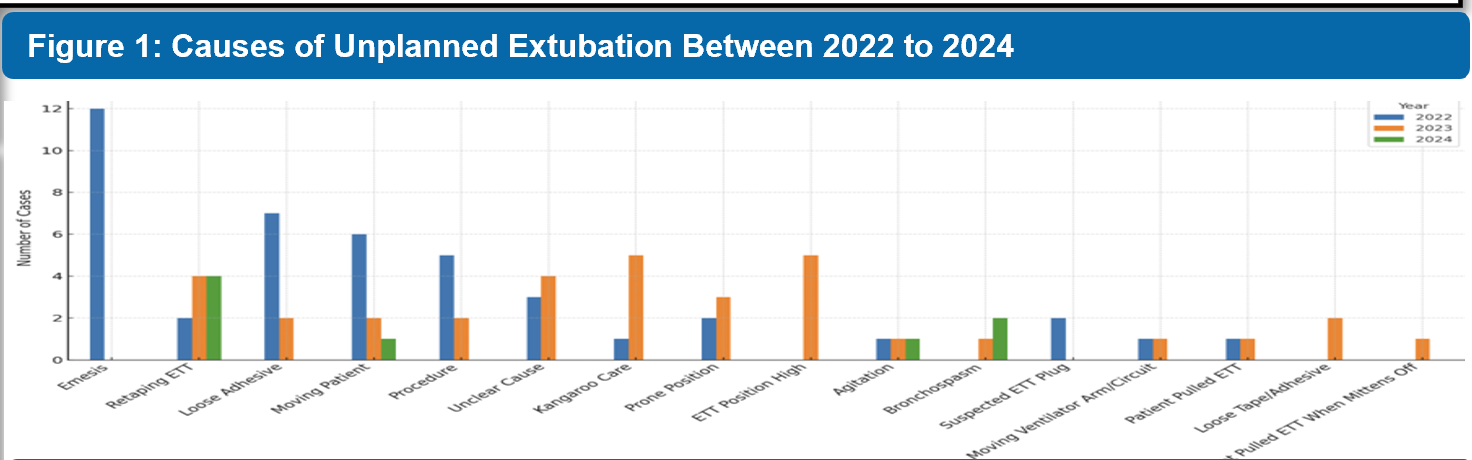
Figure 1: Causes of Unplanned Extubation Between 2022 to 2024
Figure 2: Unplanned Extubation Rate in NICU Across Nine PDSA Cycles

 Credit")