Session: Adolescent Medicine 4: Eating Disorders & Mental Health
262 - Improving Management of Patients with Suspected Eating Disorders Presenting to the Pediatric Emergency Department
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3252.262
Noah Manning, UMass Memorial Children's Medical Center, Framingham, MA, United States; Annelie W. H.. Leith, UMass Memorial Children's Medical Center, Worcester, MA, United States; Sydney Hartman-Munick, UMass Memorial Children's Medical Center, Worcester, MA, United States
Resident Physician UMass Memorial Children's Medical Center Framingham, Massachusetts, United States
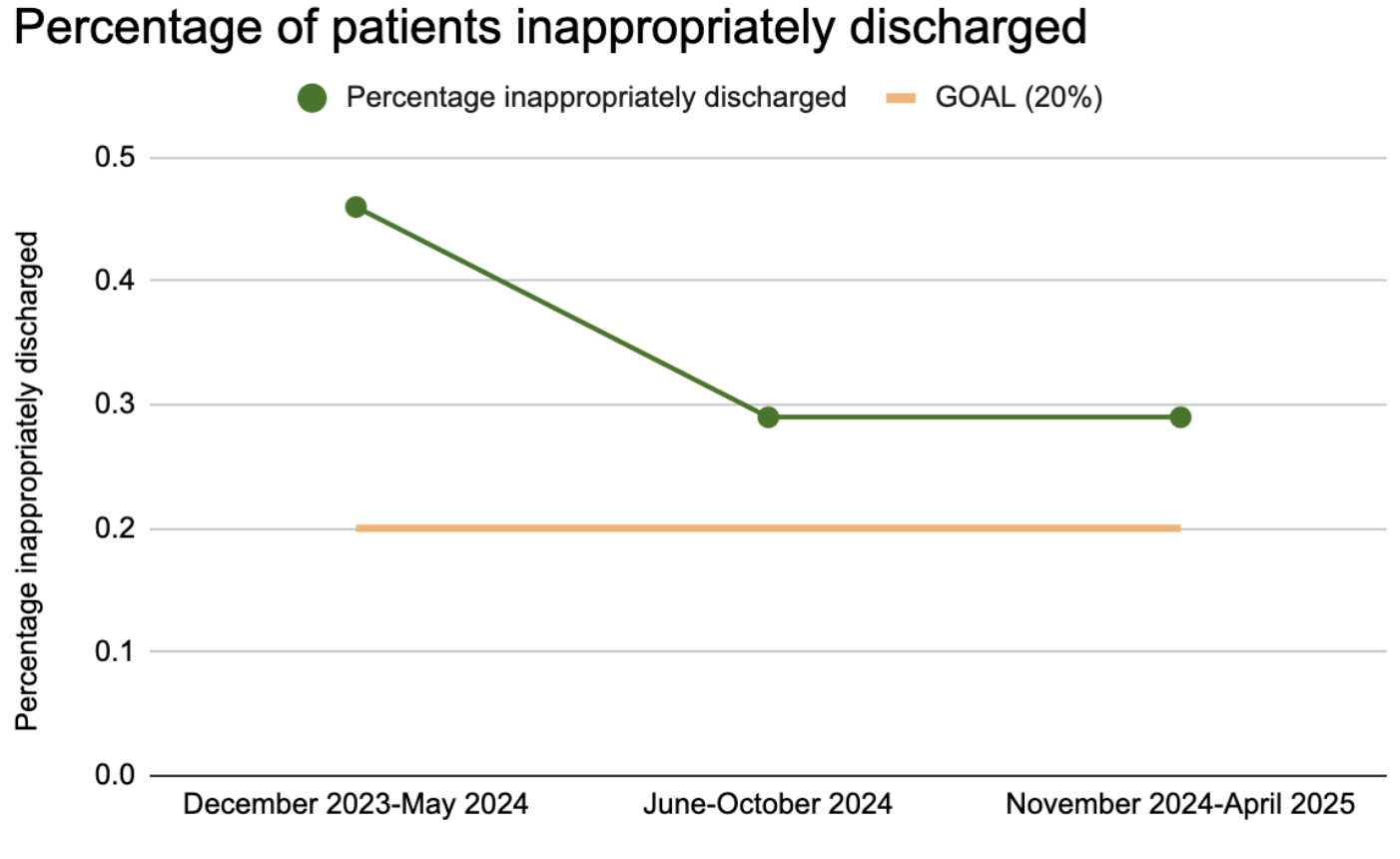
Background: Since the COVID pandemic, the burden of adolescent eating disorders (EDOs) has grown. At our academic center, we observed that patients presenting to the pediatric emergency department (PED) with concern for EDOs are often not receiving a full workup for concerning symptoms, or being discharged after meeting admission criteria, leading to delays in definitive care. Objective: By April 2026, we aim to decrease the percentage of patients inappropriately discharged (defined as being discharged without a complete work up or despite meeting admission criteria) from the PED after presenting with symptoms concerning for EDO to < 20%. Our secondary aim is to increase the percentage of residents working in the PED who report comfort with the workup of an EDO and admission criteria to >50%. Design/Methods: We performed a retrospective electronic medical record (EMR) review of patients ages 10-17 presenting to our PED in the prior 6 months, with diagnoses concerning for EDO such as "acute food refusal," "bradycardia," and "syncope." We included patients whose HPI was consistent with an EDO, and identified those who were inappropriately discharged. We then surveyed emergency medicine (EM), pediatrics, and internal medicine-pediatrics (MedPeds) residents on their knowledge of EDO workup and admission criteria.
Employing LEAN methodology, we identified a root cause as lack of standardized workup and admission criteria, then created an algorithm and EMR orderset for use in the PED to address this gap. Six months after implementation we performed an identical retrospective chart review to assess condition change.
To address knowledge gaps, we provided education to EM, pediatrics, and MedPeds residents on the need for full workup of these patients and how to use the orderset in the PED. Results: Prior to our orderset, 25% of patients received a full workup and 46% were inappropriately discharged. After our first PDSA cycle, 33% of patients received a full workup and 29% were inappropriately discharged. On a survey prior to the education, 42% of residents reported familiarity with the workup of an EDO and 33% reported knowing when to admit a patient. After education, 82% of residents reported familiarity with workup components and 82% reported familiarity with admission criteria.
Conclusion(s): Implementing an orderset with admission criteria for management of suspected EDO in the PED has led to more patients receiving full EDO workups, fewer patients inappropriately discharged, and greater provider comfort. Future PDSA cycles will focus on education of PED nurses and attendings.

 photo")