Session: Neonatal General 7: Cardiology and Hemodynamics
442 - Examination of Patent Ductus Arteriosus Diameter and Medical Therapy in the First Week of Life and the Impact on Acute Kidney Injury in Premature Neonates
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3427.442
Morgan Albert, University of Rochester School of Medicine and Dentistry, Fairport, NY, United States; Ronnie Guillet, Golisano Children's Hospital at The University of Rochester Medical Center, Greensboro, GA, United States; Hongyue Wang, University of Rochester School of Medicine and Dentistry, Rochester, NY, United States; Jonathan Burris, University of Rochester School of Medicine and Dentistry, Rochester, NY, United States
NICU Fellow University of Rochester School of Medicine and Dentistry Fairport, New York, United States
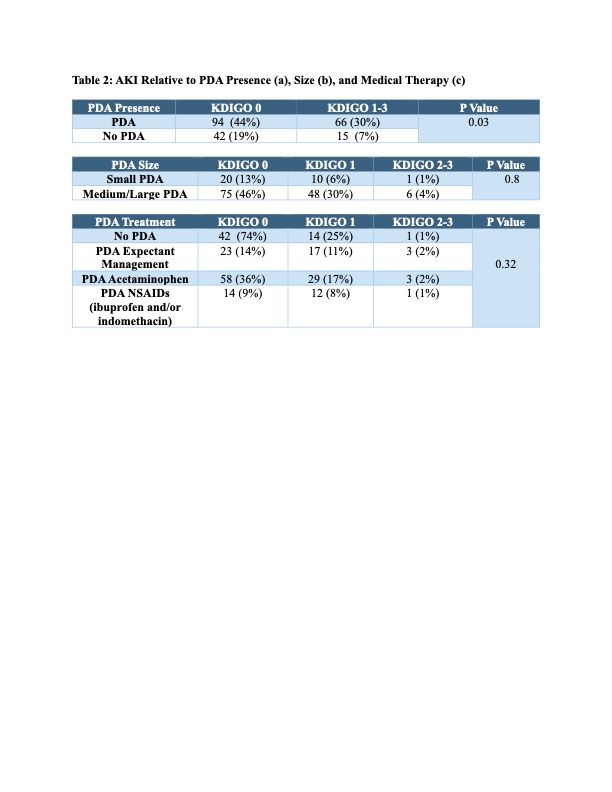
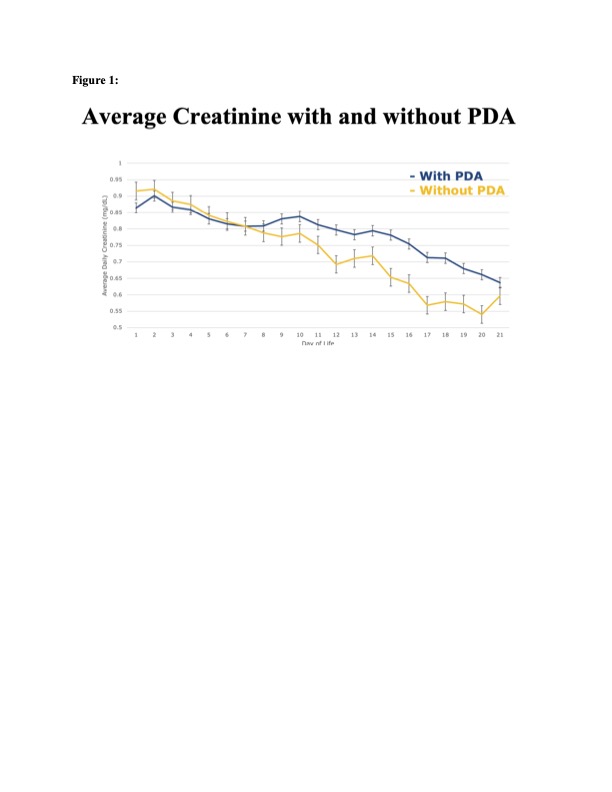
Background: Acute kidney injury (AKI) in premature low birth weight neonates increases the risk of morbidity and mortality. A hemodynamically significant patent ductus arteriosus (PDA) and the medical therapies used to close the PDA may affect neonatal kidney function. While the association between AKI and PDA management has been evaluated in the past, this study includes data on the timing of diagnosis, echocardiographic findings including ductal diameter, and treatment of PDA. Objective: Examine the relationship between PDA ductal diameter, medical management and incidence and severity of AKI in neonates born < 27 weeks' gestation (GA). Design/Methods: Retrospective cohort study of 217 infants born < 27 weeks GA at a single level IV neonatal intensive care unit 1/1/2019 - 12/31/2023. Patient clinical characteristics, daily creatinine, weights, and fluid balance over the first 21 days of life (DOL) were analyzed. PDA ductal diameter obtained as standard of care at 3 to 6 DOL and medical management for PDA closure were extracted from the medical record. Ductal diameter size was defined as small (0.1-1.4mm), medium (1.5-3mm) and large(>3mm). AKI was classified based on the modified neonatal KDIGO criteria. Morbidity included invasive ventilation at 7 and 14 DOL, bronchopulmonary dysplasia at 36 weeks corrected GA, and hypertension prior to discharge. Analysis utilized chi-square, Fischer's Exact, and analysis of variance. Results: Mean gestational age of 24-25 weeks GA between groups with and without PDA and with and without AKI were similar. Neonates with a PDA vs no PDA were of lower mean birthweight (749g vs 777g). Daily creatinine rose to statistically higher values from DOL 9 to 20 in those with PDA compared to no PDA (Figure 1). Neonates with a PDA following birth were more likely have vasopressor support in the first 21 DOL (p=0.01), be on invasive ventilation at 7 DOL (p < 0.01) and 14 DOL (p < 0.01) and have BPD (p < 0.01) compared to no PDA (Table 1). There was no difference in hypertension at 36 weeks corrected GA or prior to discharge (p=0.24) Neonates with a PDA were more likely to have any stage of AKI (p=0.03) (Table 2a). There was no difference in AKI severity with respect to PDA size (p=0.79) (Table 2b), or AKI incidence based on initial medical management of PDA (acetaminophen vs ibuprofen vs expectant) (p=0.32) (Table 2c).
Conclusion(s): PDA diameter on DOL 3-6 was not associated with risk for AKI. We confirmed that any PDA is associated with AKI, need for invasive ventilation through the 14 days, and need for vasopressor support. Further analysis of day-specific PDA diameter is required.
Table 1. Demographics
Table 2. AKI Relative to PDA Presence (a), Size (b), and Medical Therapy (c)

.jpg "Morgan Albert, DO (she/her/hers) photo")
.jpg)