554 - One-year mortality among infants with an Apgar score of zero at 10 minutes
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3535.554
Ida Lagerström, Karolinska Institutet, Dep of Medicine Solna, Stockholm, Stockholms Lan, Sweden; Jonas Söderling, Karolinska Institutet, Stockholm, Stockholms Lan, Sweden; Neda Razaz, Karolinska Institutet, Stockholm, Stockholms Lan, Sweden; Maria Altman, Karolinska Institutet, Stockholm, Stockholms Lan, Sweden; Stefan Johansson, Karolinska Institutet, Stockholm, Stockholms Lan, Sweden; Jenny Bolk, Karolinska Institutet, Stockholm, Stockholms Lan, Sweden
Resident doctor Karolinska Institutet, Dep of Medicine Solna Stockholm, Stockholms Lan, Sweden
Background: Infants with an Apgar score of 0 at 10 minutes are considered to have a poor prognosis with high mortality rates. Consequently, an Apgar score of 0 at 10 minutes has previously been used as a criterion in determining when to discontinue neonatal resuscitation. Current guidelines on when to discontinue resuscitation in infants with very low Apgar scores are based on very low-certainty evidence, due to heterogeneity among the studies and small sample sizes. Contemporary population-based data are needed to improve knowledge of mortality rates, refine resuscitation guidelines, and support clinical decision-making and parental counseling. Objective: To examine overall one-year mortality and cause-specific mortality in infants with Apgar score 0 at 10 minutes after birth compared with Apgar scores of 1, 2, or 3. Design/Methods: This nationwide population-based cohort study included all 2 395 247 singleton live births at ≥36 weeks gestation in Sweden, between 1 January 1999 and December 31 2021. Data were collected through national registries. A total of 1397 infants with an Apgar score of 0-3 at 10 minutes were included in the study. The exposure was an Apgar score of 0 at 10 minutes after birth. The main outcome was mortality within one year after birth, and the secondary outcome was cause-specific mortality. A modified Poisson regression model was used to calculate risk ratios with 95% confidence intervals. The analyses were adjusted for several maternal, infant and socioeconomic confounders. Results: Among the 1397 infants included (760/1397 [54.4%] boys), the one-year mortality rate was 126/245 (51.4%) for infants with an Apgar score of 0 compared to 130/275 (47.3%), 71/344 (20.6%) and 97/533 (18.2%) for infants with Apgar scores of 1, 2 and 3, respectively. The adjusted risk ratios for one-year mortality were 2.79 (95% CI, 2.13-3.65) for score 0, 2.49 (95% CI, 1.91-3.25) for score 1, and 1.09 (95% CI, 0.80-1.49) for score 2, compared with infants with Apgar score 3. Asphyxia-related diagnoses were the most common cause of death, followed by congenital abnormalities.
Conclusion(s): In this study, infants with Apgar score 0 at 10 minutes had similar one-year mortality rates to those with an Apgar score of 1, but higher rates compared to infants with Apgar scores of 2 or 3. These findings suggest that infants with Apgar scores of 0 and 1 have comparable risks of death and that distinguishing between these scores may have limited prognostic value for resuscitation decisions.

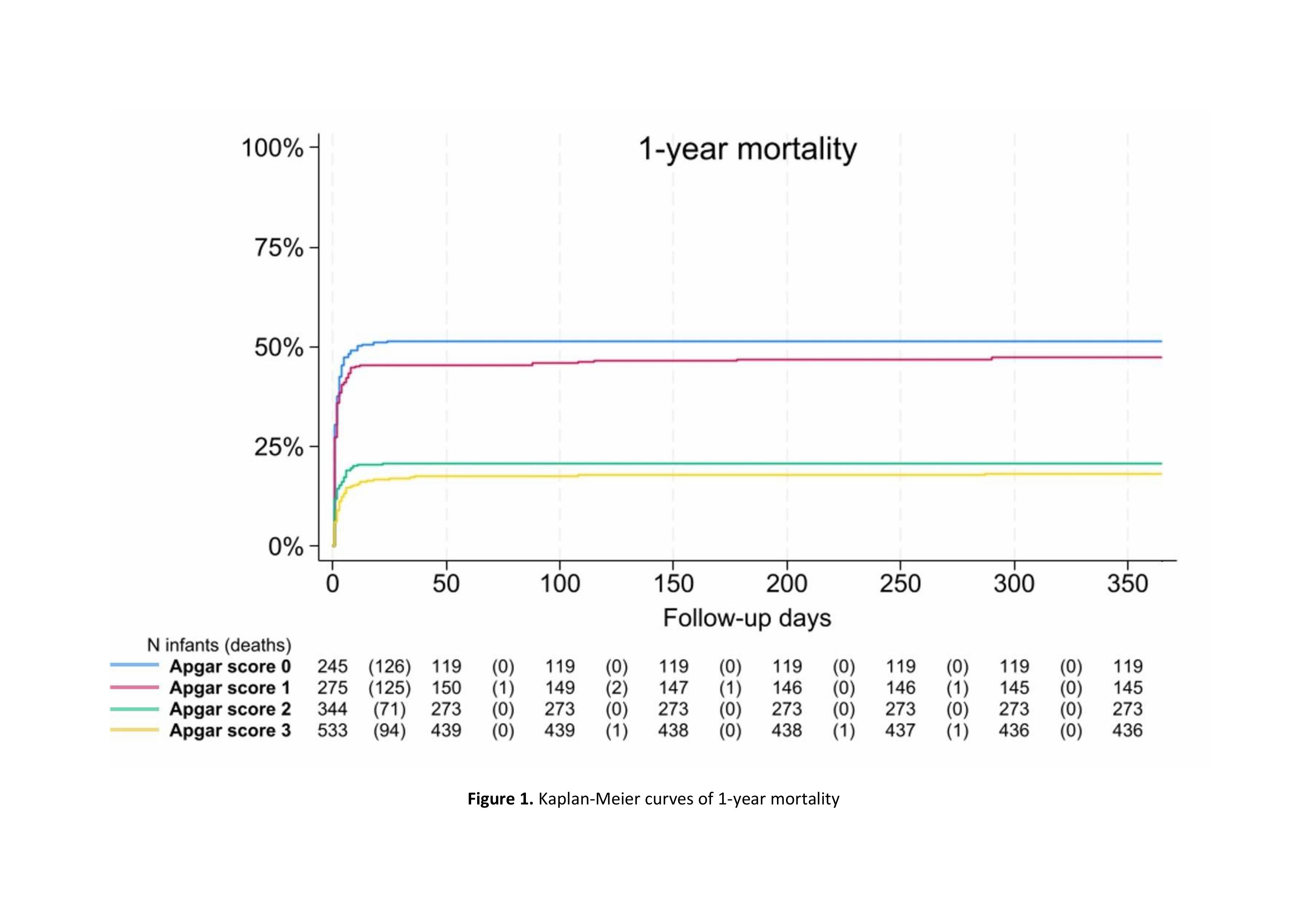 Kaplan-Meier curves of 1-year mortality
Kaplan-Meier curves of 1-year mortality