709 - Ocular Point-of-Care Ultrasound and Nonmydriatic Fundus Photography for Evaluation of Papilledema in the Pediatric Emergency Department
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3686.709
Emily Berner, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Sydney C. Clark, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Laura Sartori, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Aaron Chen, Childrens Hospital of Philadelphia, Bala Cynwyd, PA, United States; Robert Avery, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Jacob T. Hemberger, Children’s Hospital of Philadelphia, Philadelphia, PA, United States; Daniel Corwin, Childrens Hospital of Philadelphia, Philadelphia, PA, United States
Fellow Physician Childrens Hospital of Philadelphia Philadelphia, Pennsylvania, United States
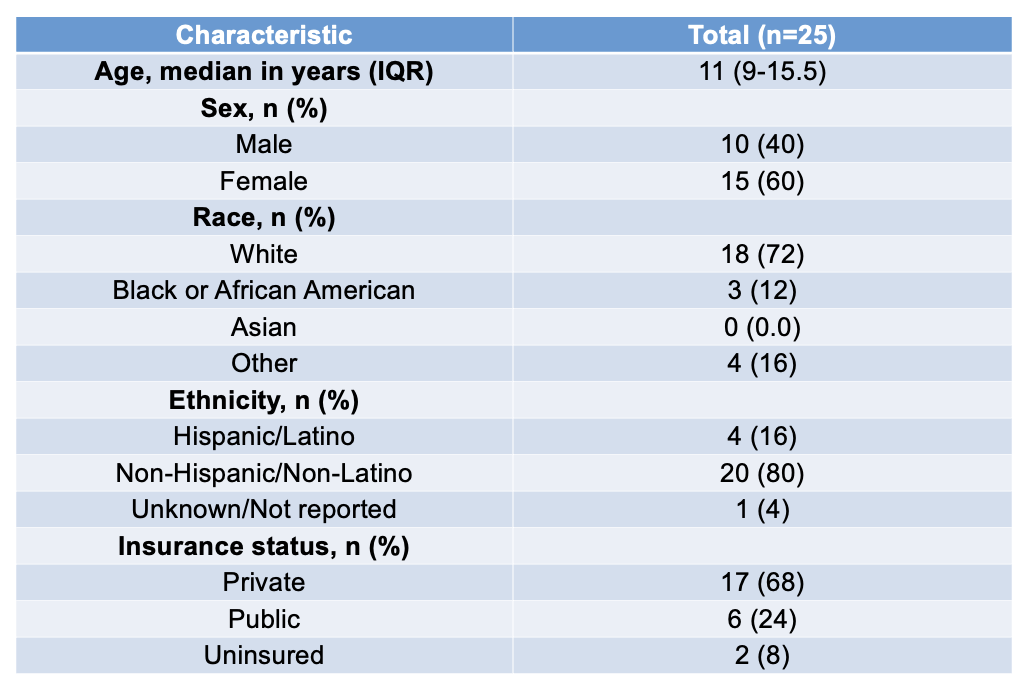
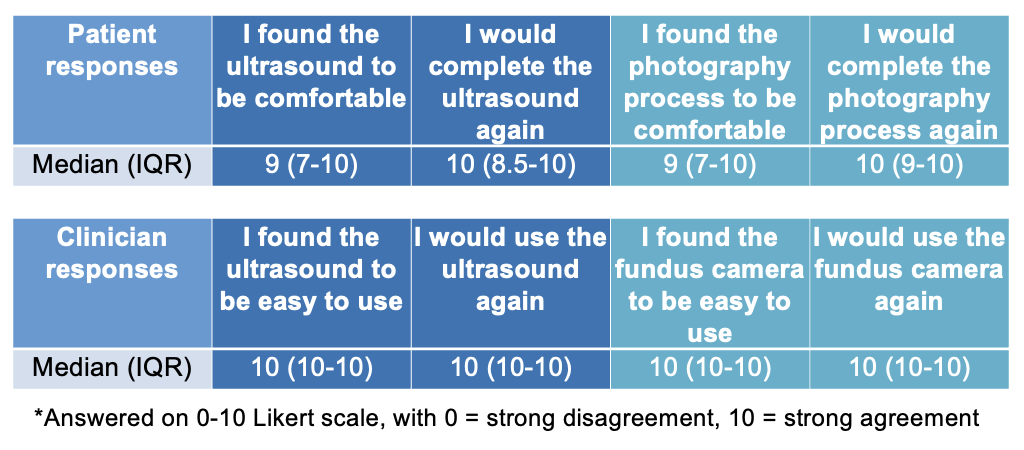
Background: Papilledema may result from life and/or vision threatening elevations in intracranial pressure (ICP). Emergent referrals for suspected elevated ICP require significant human and imaging resources. Indirect ophthalmoscopy by an ophthalmologist is currently the gold standard for evaluation of papilledema, however can result in prolonged emergency department (ED) stays or even require transfer to a tertiary care facility. Recently, ocular point-of-care ultrasound (POCUS) and nonmydriatric fundus photography (NFP) are two strategies that enable non-ophthalmologists to determine if papilledema is present or absent. Our study examined the feasibility and accuracy of ocular POCUS and NFP by non-ophthalmologists to evaluate for papilledema. Objective: Our primary outcome was percent of participants for whom ocular POCUS and NFP was interpretable. Design/Methods: We prospectively recruited children age 3-17 years presenting to a large tertiary care pediatric ED for whom ophthalmology was consulted to evaluate for papilledema. We excluded those with ocular trauma or infection. Participants underwent ocular POCUS and NFP by trained pediatric emergency medicine (PEM) clinicians in addition to dilated ophthalmologic exam. Following study procedures, we administered surveys assessing feasibility to participants and clinicians performing study procedures. Ultrasound images were reviewed retrospectively by a masked PEM physician with subspecialty training in pediatric ultrasound, and fundoscopic photos were reviewed retrospectively by a masked pediatric neuro-ophthalmologist, to determine both interpretability as well as clinical findings. Results: We enrolled 25 participants between August 2024-August 2025; participant demographics are summarized in Table 1. In total, 24/25 (96%) had interpretable ocular POCUS and 24/25 (96%) had interpretable NFP. Patients found both POCUS and NFP to be very comfortable, and clinicians found both POCUS and NFP very easy to use (Table 2). Kappa between POCUS and NFP was 0.44. Sensitivity and specificity were 0.93 and 0.80 for POCUS, and 0.64 and 0.90 for NFP.
Conclusion(s): Our preliminary results suggest that ocular POCUS and NFP are tolerable for pediatric patients and easy to use for providers in the ED, representing feasible alternative evaluation techniques for papilledema in the pediatric ED setting. Our analysis exhibited moderate agreement between POCUS and NFP, and reasonable Se and Sp compared to a dilated ophthalmology fundoscopic exam. Our current results are limited by small sample size, but additional enrollment of study participants is ongoing.