572 - Resuscitation characteristics before and after transition from Neonatal Resuscitation Program® (NRP) to Pediatric Advanced Life Support (PALS) as default resuscitation algorithm in a Level IV NICU
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3553.572
Mary Haggerty, Children's Hospital of Philadelphia, haddonfield, NJ, United States; Kristen Coletti, Children's Hospital of Philadelphia, Wynnewood, PA, United States; Heidi M. Herrick, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Lauren Heimall, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Laura Sillers, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Anne Ades, Childrens Hospital of Philadelphia, Philadelphia, PA, United States
Attending Neonatologist Children's Hospital of Philadelphia haddonfield, New Jersey, United States
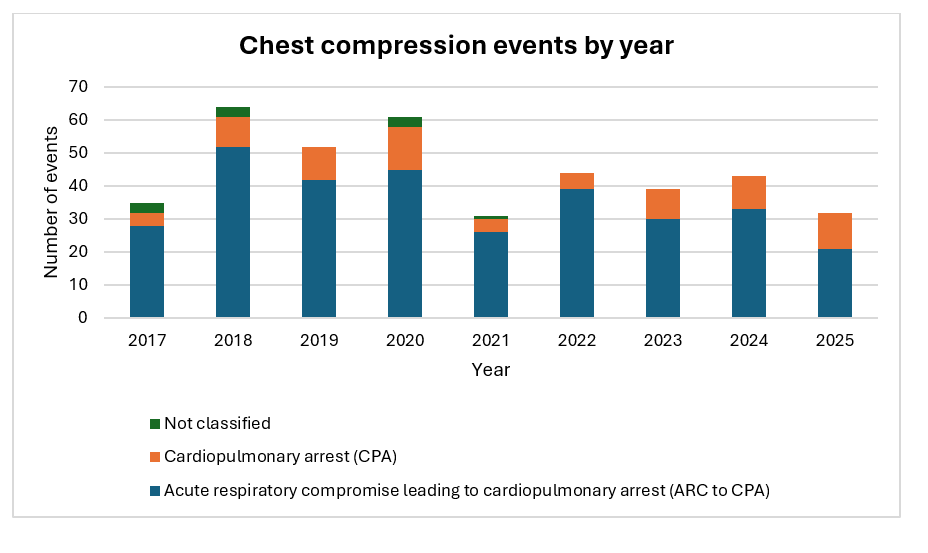
Background: Critical knowledge gaps remain around optimal resuscitation practices for hospitalized neonates and infants. No universal recommendation for timing of transition from neonatal to pediatric guidelines exists. Prior to 2021, the NICU at Children's Hospital of Philadelphia defaulted to NRP guidelines for in-hospital NICU cardiac arrest. PALS guidelines were utilized at the resuscitation leader's discretion based on patient age or physiology. In 2021, the NICU transitioned to PALS guidelines as the default resuscitation algorithm. This transition occurred over 2 years with all providers completing PALS training by September 2023. Objective: To describe resuscitation practices and short-term outcomes of NICU cardiac arrests before and after transition to PALS. Design/Methods: Retrospective observational pre-and-post study of patients with cardiac arrest between 1/1/17 and 10/27/25. Cardiac arrest was defined as receipt of chest compressions of any duration. Patients and resuscitation characteristics were identified in a hospital and unit-specific QI resuscitation database. Descriptive statistics were used to analyze resuscitation practices and outcomes. Chi-square tests were used to compare CPR duration and outcomes. Results: There were 240 CPR events in the pre-transition period (1/2017 to 9/2021, 57 months) and 162 events in the post-transition period (10/2021 to 10/2025, 48 months). The CPR rate per study period day was higher in the pre-transition period (0.138 per day vs 0.108 per day). There was a higher percentage of short CPR events (1 to 5 minutes of CPR) in the pre-transition period (p < 0.001). There was a higher percentage of longer CPR events (11 to 20 minutes, p=0.008, and greater than 20 minutes, p=0.02) in the post-transition period. Return of spontaneous circulation (ROSC) was higher in the pre-transition period (p < 0.001).
Conclusion(s): In the 4 -year period after transition to PALS as the default resuscitation algorithm, the rate of CPR was lower. There was a trend toward longer CPR events and decreased rates of ROSC. Pre-cardiac arrest illness severity, resuscitation factors, changes in families' goals of care, and other factors that may impact outcomes were not accounted for and should be examined in future studies.
Figure 1. Number and type of chest compression events per year

.jpg)
