508 - Real-World Impact of RSV Immunoprophylaxis on Illness Burden and Healthcare Utilization in Infants Across Two Seasons
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3489.508
Andrea Rivera-Sepulveda, Nemours Children's Hospital, ORLANDO, FL, United States; Sobur Ali, University of Central Florida, Orlando, FL, United States; Kayla Morrell, Nemours Children's Hospital, Wilmington, DE, United States; Jonathan M. Miller, Nemours Children's Hospital, Delaware, Wilmington, DE, United States; Joshua Katz, Nemours Children's Hospital, Orlando, FL, United States; Kristin Maiden, Nemours Children's Hospital, Wilmington, DE, United States; Sara Slovin, Nemours Children's Hospital, Wilmington, DE, United States; Zhongcui Gao, Nemours Children's Hospital, Lancaster, PA, United States; Danielle Burns, Nemours Children's Hospital, Bel Air, MD, United States; Taj Azarian, University of Central Florida College of Medicine, Orlando, FL, United States
Associate Professor Nemours Children's Hospital ORLANDO, Florida, United States
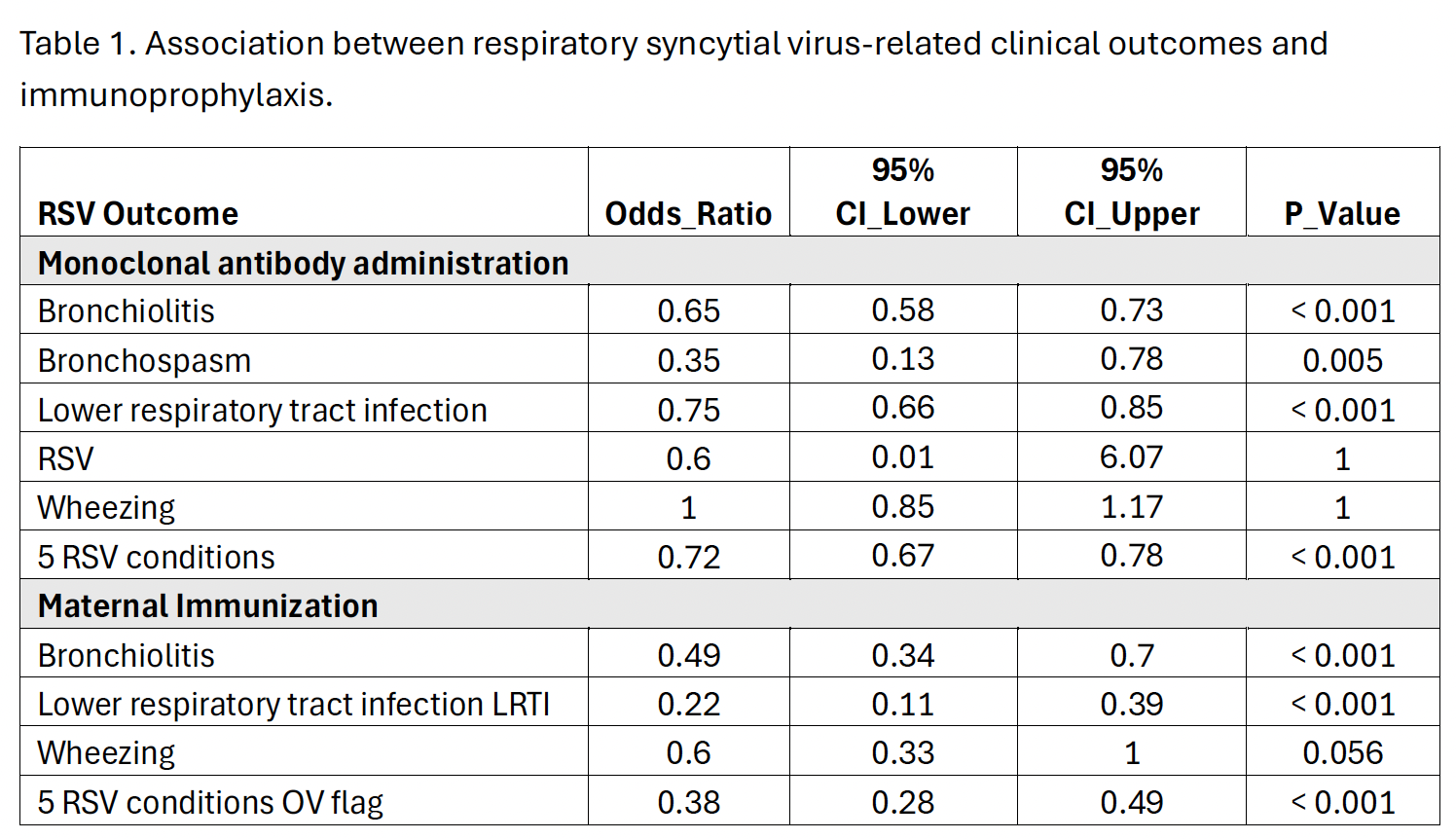
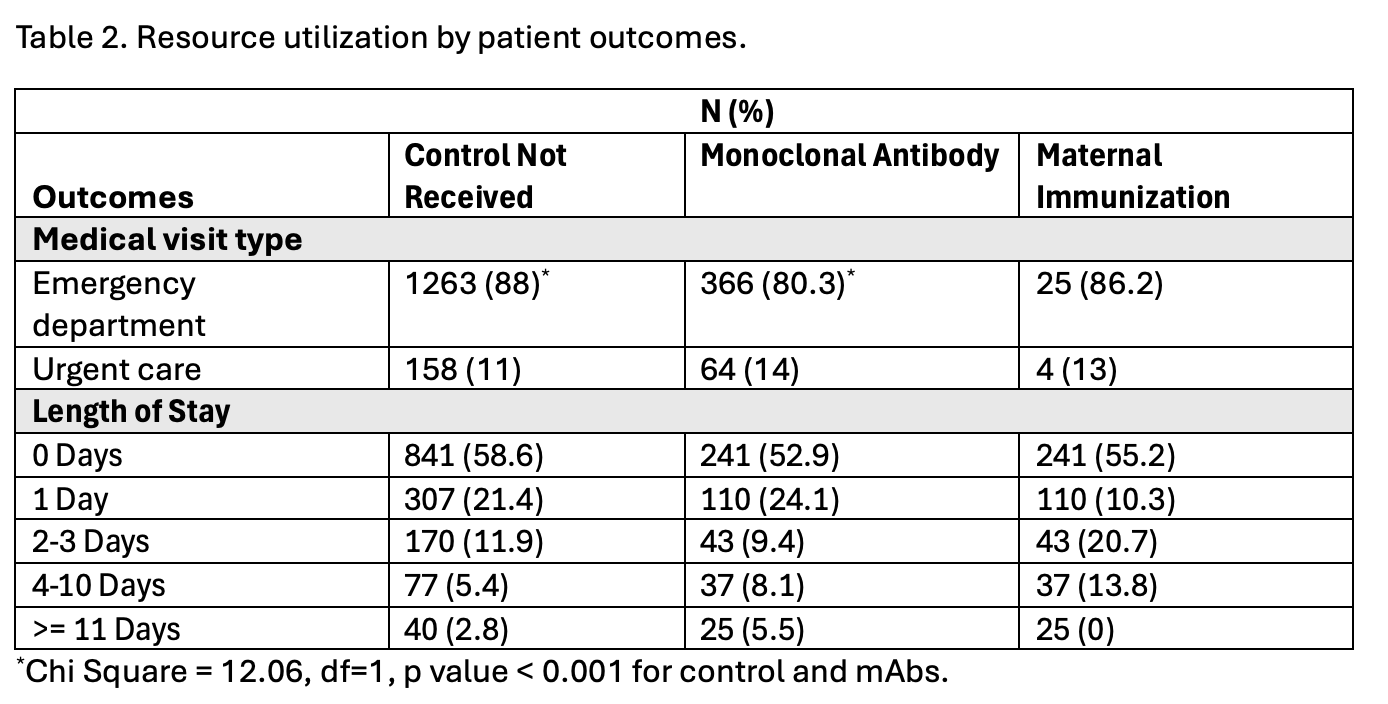
Background: Respiratory syncytial virus (RSV) continues to drive substantial emergency and inpatient resource use among infants. The introduction of maternal RSV vaccination and monoclonal antibody (mAb) prophylaxis in 2023 offers opportunities to mitigate this burden. While efficacy has been established in controlled trials, comparative real-world data on healthcare utilization among prophylaxis groups remains limited. Objective: To compare illness burden and healthcare utilization among infants who received RSV prophylaxis, including maternal RSV vaccination, mAb, or both, versus those without prophylaxis across two consecutive RSV seasons. Design/Methods: A retrospective cohort study was conducted using a pediatric healthcare network across two states. We analyzed electronic medical records for infants 0 to 19 months born between February 2023 and March 2025. Encounters were classified into four groups: no prophylaxis, mAb, maternal RSV vaccination, or both. RSV-related encounters were identified through the International Classification of Diseases, tenth edition (ICD-10) codes for bronchiolitis, lower respiratory tract infection (LRTI), or wheezing. Outcomes included emergency department (ED) visits, hospitalizations, and length of stay. Group comparisons used chi-square or Fisher's exact tests, and Cox proportional hazards models estimated relative illness risk over time. Results: Among a cohort of 23,249 infants, prophylaxis groups demonstrated significantly lower RSV-associated illness compared with unprotected infants. mAb recipients had reduced odds of bronchiolitis (OR 0.65, 95% CI 0.58-0.73, p< 0.001), bronchospasm (OR 0.35, p=0.005), and LRTI (OR 0.75, p< 0.001). Maternal vaccination conferred further protection against bronchiolitis (OR 0.49, p< 0.001) and LRTI (OR 0.22, p< 0.001). ED-initiated admissions were highest among unprotected infants (88%) versus mAbs (80%, p< 0.001). Prolonged admissions (>10 days) occurred more often without prophylaxis (2.8%) than with mAbs (5.5%) or maternal vaccination (0%). Overall, both strategies were associated with lower RSV morbidity and fewer acute-care encounters.
Conclusion(s): In this large, real-world cohort, both maternal RSV vaccination and infant mAb prophylaxis were associated with reduced RSV-related illness and healthcare utilization across two seasons. These findings support early adoption of RSV preventive strategies to lessen acute respiratory morbidity and resource demands in pediatric populations.
Association between respiratory syncytial virus-related clinical outcomes and immunoprophylaxis.
Table 2. Resource utilization by patient outcomes.