Session: Mental Health 3: Interventions and Clinical Integration
281 - Implementation outcomes from Paloma: A suicide prevention intervention for Spanish-speaking parents delivered by CHWs by referral from pediatric primary care
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3270.281
Sarah Polk, Johns Hopkins University School of Medicine, Baltimore, MD, United States; Ellen Molino, Johns Hopkins University, Baltimore, MD, United States; Kaimy Torres-Hernandez, Johns Hopkins University, Baltimore, MD, United States; Bev Rosario Williams, Johns Hopkins Bloomberg School of Public Health, Atlanta, GA, United States; Isabella Perea caicedo, New York Medical College, New York, NY, United States; Laura Prichett, Johns Hopkins School of Medicine, Baltimore, MD, United States; Amanda Finney, Johns Hopkins University School of Medicine, Columbia, MD, United States
Associate Professor of Pediatrics Johns Hopkins University School of Medicine Baltimore, Maryland, United States
Background: Pediatric primary care is an important venue in which to identify and mitigate suicide risk. Latinx youth in immigrant families are vulnerable to increased risk of suicidal ideation when exposed to immigration-related stressors and structural barriers to mental health care access.
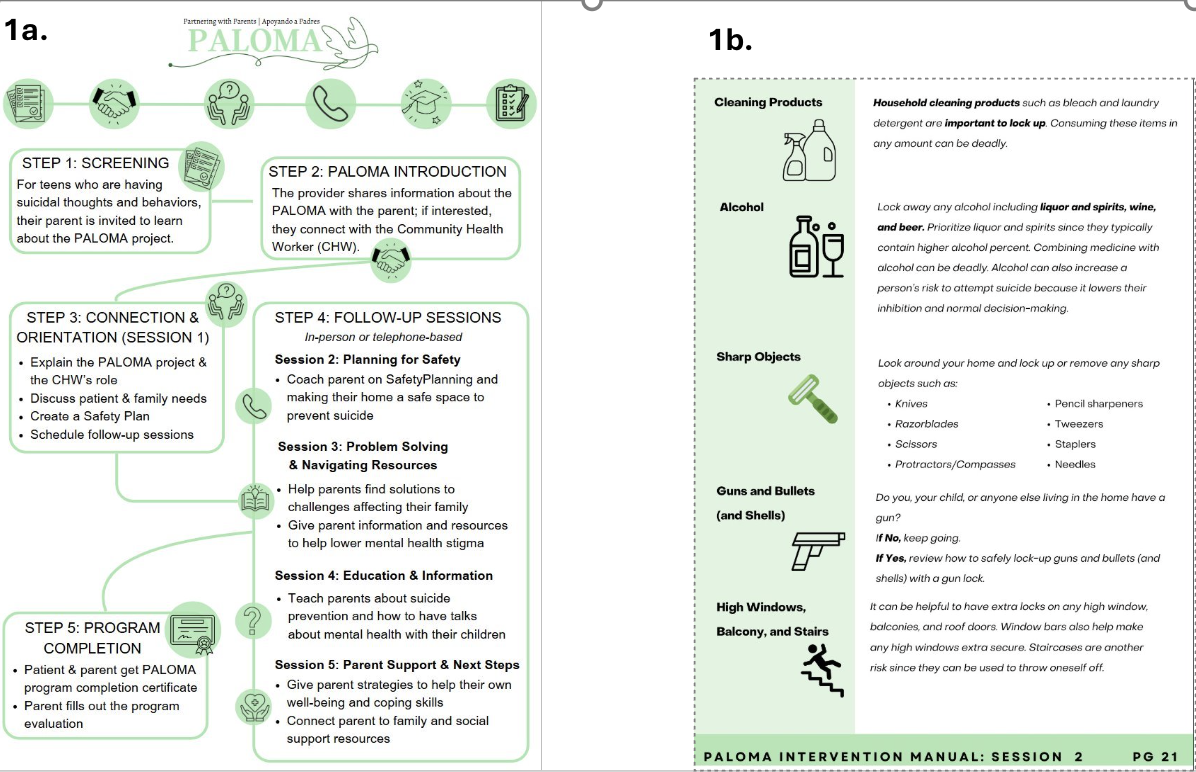
We developed the Paloma intervention for Spanish-speaking parents of youth experiencing suicidal ideation and behavior referred by their pediatrician. Paloma consists of 5 phone calls delivered by a community health worker. It complements pediatric care by bolstering parental self-efficacy to manage suicidal ideation and behaviors (Figure 1).
A pragmatic clinical trial of Paloma at 3 pediatric primary care practices in Baltimore, MD is ongoing. Data collection for the pilot trial includes process measures and qualitative data from participating parents and referring pediatric providers. Objective: To describe the implementation outcomes of a pragmatic pilot trial of the Paloma suicide prevention intervention. Design/Methods: Process measures include the number of referrals, referrals accepted and intervention attendance. We captured rates and results of the PHQ-A from the electronic medical record prior to and during the trial. We have analyzed PHQ-A data using descriptive statistics and will apply linear regression models.
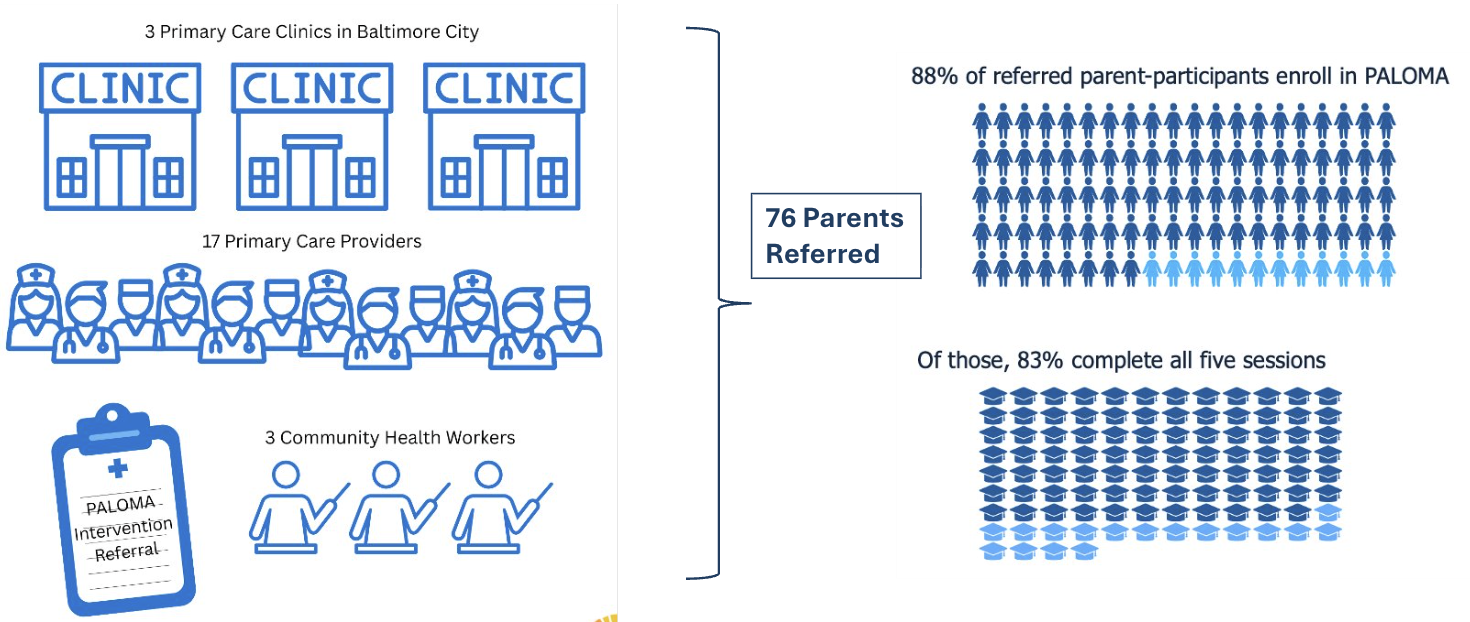
We conducted semi-structured interviews with pediatric providers regarding their experience with Paloma and challenges and opportunities to safety planning. We are analyzing the interviews using Rapid Qualitative Analysis. Results: As of September 30, 2025, we had 76 referrals from 17 pediatric providers at 3 clinics. 88% of referred parents (n=67) enrolled in the intervention of whom 83% completed all intervention sessions (Figure 2). Of enrolled intervention participants, 85% (n=57) consented to research participation. Pilot trial enrollment is complete.
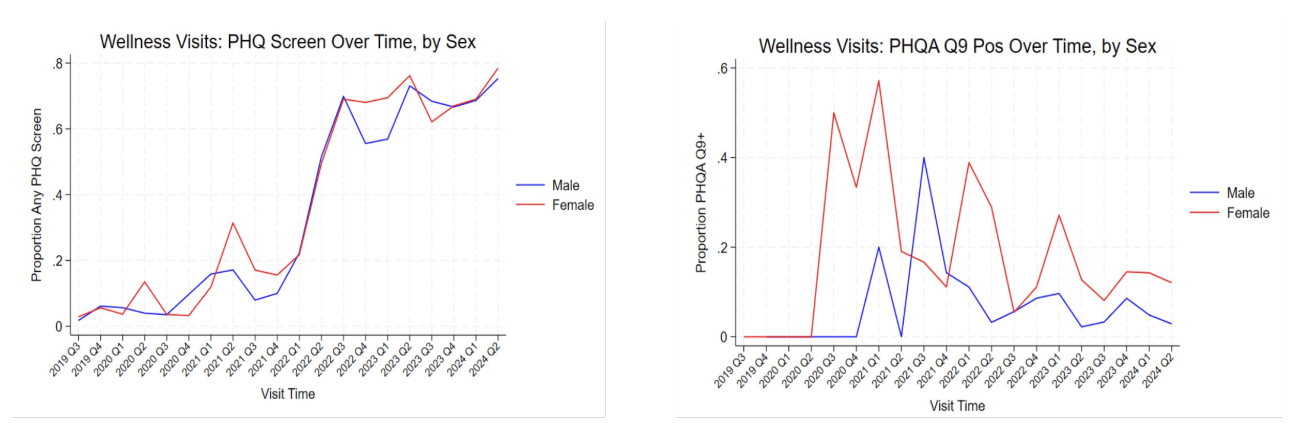
We have extracted 2 years of screening and visit diagnosis code from the electronic medical record. Analysis is underway (Figure 3).
We conducted semi-structured interviews with 18 pediatric providers representing all 3 participating practices. Rapid qualitative analysis is underway. Regarding the role of Paloma, one pediatrician shared, "Well, right now we have Paloma which is very helpful. [it] helps parents also feel supported, because ... mostly the services are focused on the teen patient."
Conclusion(s): Quantitative and qualitative implementation outcome data to date from our pilot study of the Paloma intervention to prevent suicide among Latine youth in immigrant families demonstrate the intervention's feasibility and acceptability.
Figure 1. Implementation materials co-designed by research team and parent advisory board for the Paloma suicide prevention intervention (1a. Storyboard for parents explaining the intervention process; 1b. Safety Planning handout from Session 2 of the parent manual)
Figure 2. Participation in the Paloma suicide prevention intervention according to role, clinic, provider, community health worker and parent participant
Figure 3. Changes in depression screening, including PHQA Question 9, over time by sex at the primary clinic site for the Paloma intervention