531 - Intratracheal Administration of Budesonide Mixed with Surfactant for Bronchopulmonary Dysplasia in Preterm Infants: A Systematic Review and Meta-analysis
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3512.531
Yohei Minamitani, Kumamoto City Hospital, Kumamoto, Kumamoto, Japan; Kana Saito, Tokai University, Isehara, Kanagawa, Japan; Naoyuki Miyahara, saitama medical center, kawagoe, Saitama, Japan; Masayo Kanai, Saitama Medical Center, Kawagoe, Saitama, Japan; Fumihiko Namba, Saitama Medical Center, Saitama Medical University, Kawagoe, Saitama, Japan
MD, PhD Kumamoto City Hospital Kumamoto, Kumamoto, Japan
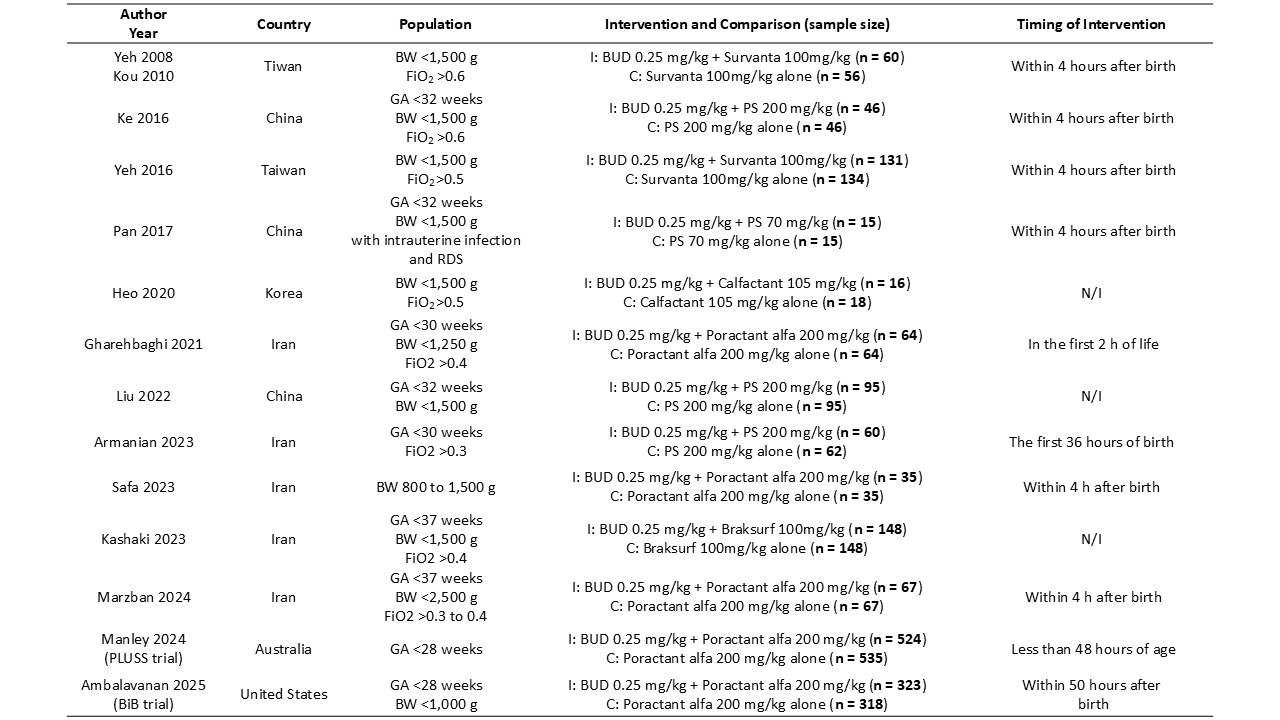
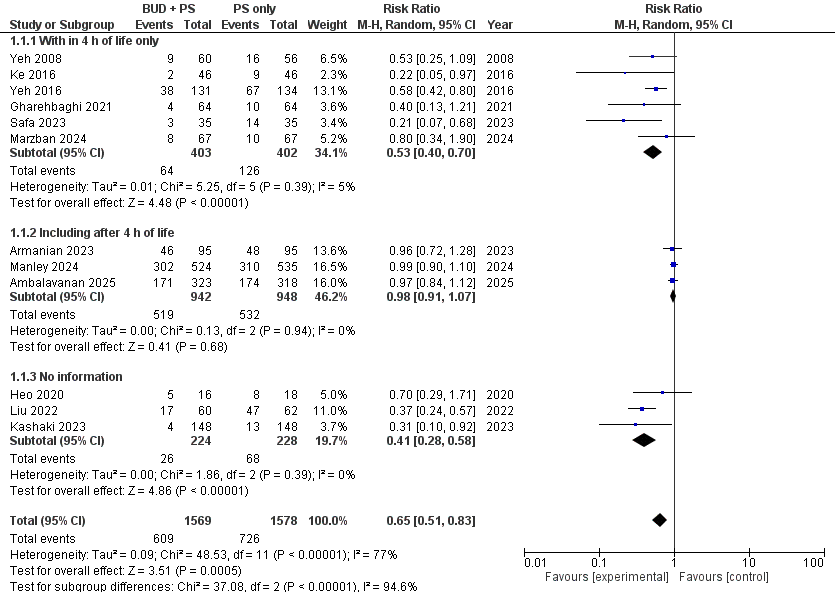
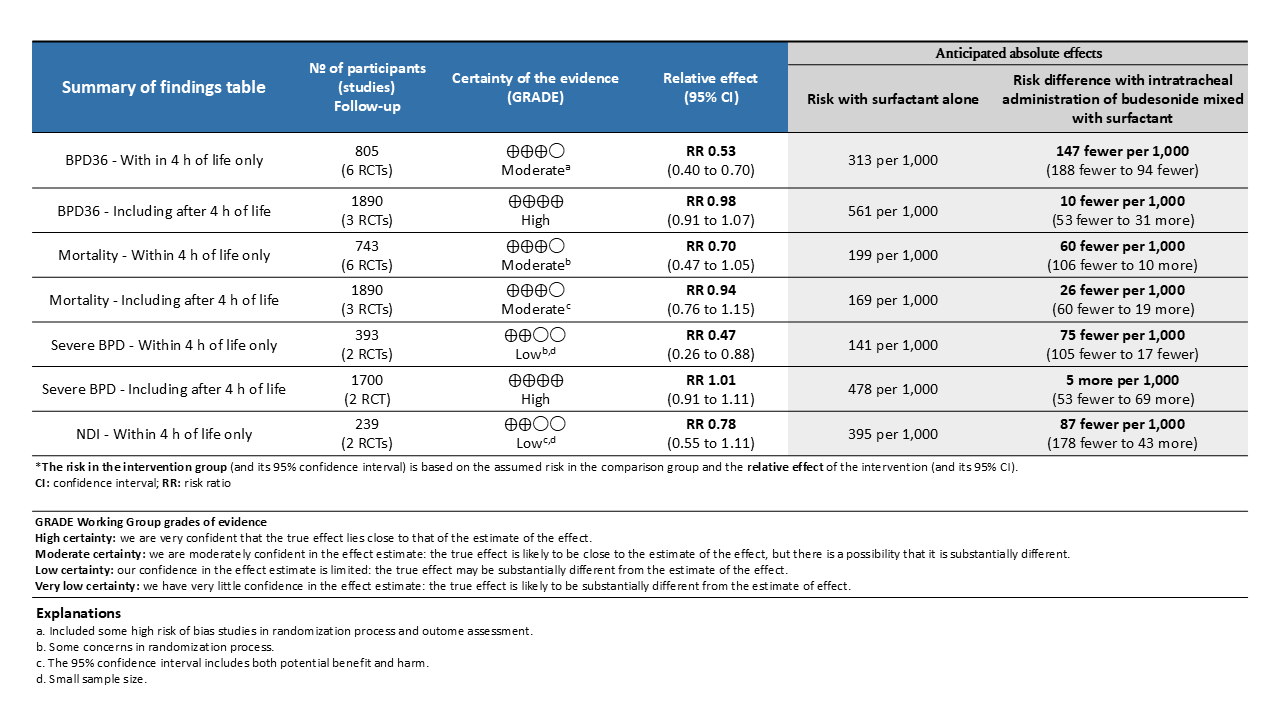
Background: Bronchopulmonary dysplasia (BPD) remains a major cause of long-term respiratory and neurodevelopmental morbidity in preterm infants. Systemic corticosteroids reduce BPD risk but may increase intestinal perforation and cerebral palsy. Several small randomized controlled trials (RCTs) have reported that intratracheal administration of budesonide (BUD) mixed with pulmonary surfactant (PS) reduces the composite outcome of BPD or death without adverse effects. However, two recent large multicenter RCTs found no significant benefit, leaving the efficacy of BUD mixed with PS uncertain. Objective: To systematically review and meta-analyze RCTs evaluating the efficacy of intratracheal BUD mixed with PS for the prevention of BPD in preterm infants. Design/Methods: A comprehensive literature search was conducted in CENTRAL, CINAHL, ClinicalTrials.gov, Embase, MEDLINE, PubMed, and WHO ICTRP on March 22, 2025, supplemented by manual searches of relevant references. Four investigators independently screened, selected, and extracted data. Eligible studies were RCTs comparing BUD + PS with PS alone in infants born at < 37 weeks' gestation. The primary outcome was BPD36, defined as the need for supplemental oxygen or respiratory support at 36 weeks' postmenstrual age (PMA). Data were pooled using random-effects meta-analysis, and the certainty of evidence was assessed with the GRADE approach. The review followed the Cochrane Handbook and PRISMA guidelines. Results: Of 267 records identified, 13 RCTs involving 3,177 infants met inclusion criteria. Overall, BUD + PS significantly reduced BPD36 compared with PS alone (n=3,147; risk ratio [RR] 0.65, 95% CI 0.51-0.83), with substantial heterogeneity (I²=77%). Subgroup analysis by timing of initial intervention revealed that BUD + PS administered within 4 hours of birth significantly reduced BPD36 (n=805; RR 0.53, 95% CI 0.40-0.70; moderate certainty), whereas no significant difference was observed in studies where the initial dose could be administered beyond 4 hours of life (n=1,890; RR 0.98, 95% CI 0.91-1.07; high certainty).
Conclusion(s): Intratracheal administration of BUD mixed with PS within 4 hours of birth may reduce the incidence of BPD, whereas no beneficial effect was found in studies where the initial dose could be administered beyond 4 hours of life. Further well-powered RCTs focusing on early intervention are warranted to clarify the optimal timing and confirm the efficacy of this strategy for BPD prevention.

 photo")