Session: Neonatal General 7: Cardiology and Hemodynamics
441 - Risk of Adverse Neonatal Outcomes in Pregnant Patients with Congenital Heart Disease (CHD)
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3426.441
Poojita Dasika, Albert Einstein College of Medicine, Santa Clara, CA, United States; Shreya Ramineni, Albert Einstein College of Medicine, Bronx, NY, United States; Diana S. Wolfe, Montefiore/Einstein, Bronx, NY, United States; Anna Bortnick, Montefiore Medical Center, Bronx, NY, United States; Daphne T. Hsu, Albert Einstein College of Medicine, Brinx, NY, United States; manoj Gupta, Children’s Hospital at Montefiore, Bronx, NY, United States
Cardiology Physician Children’s Hospital at Montefiore Bronx, New York, United States
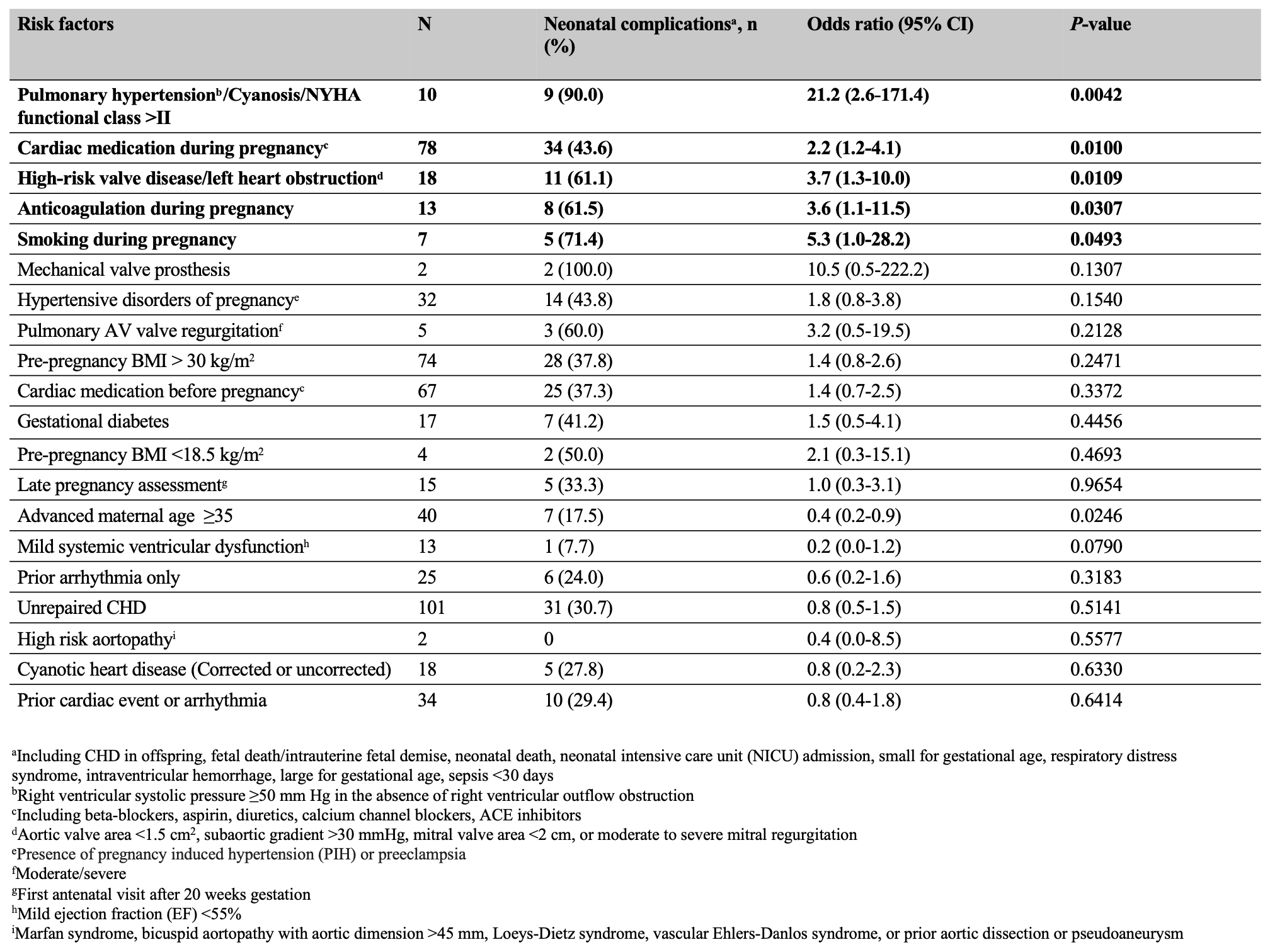
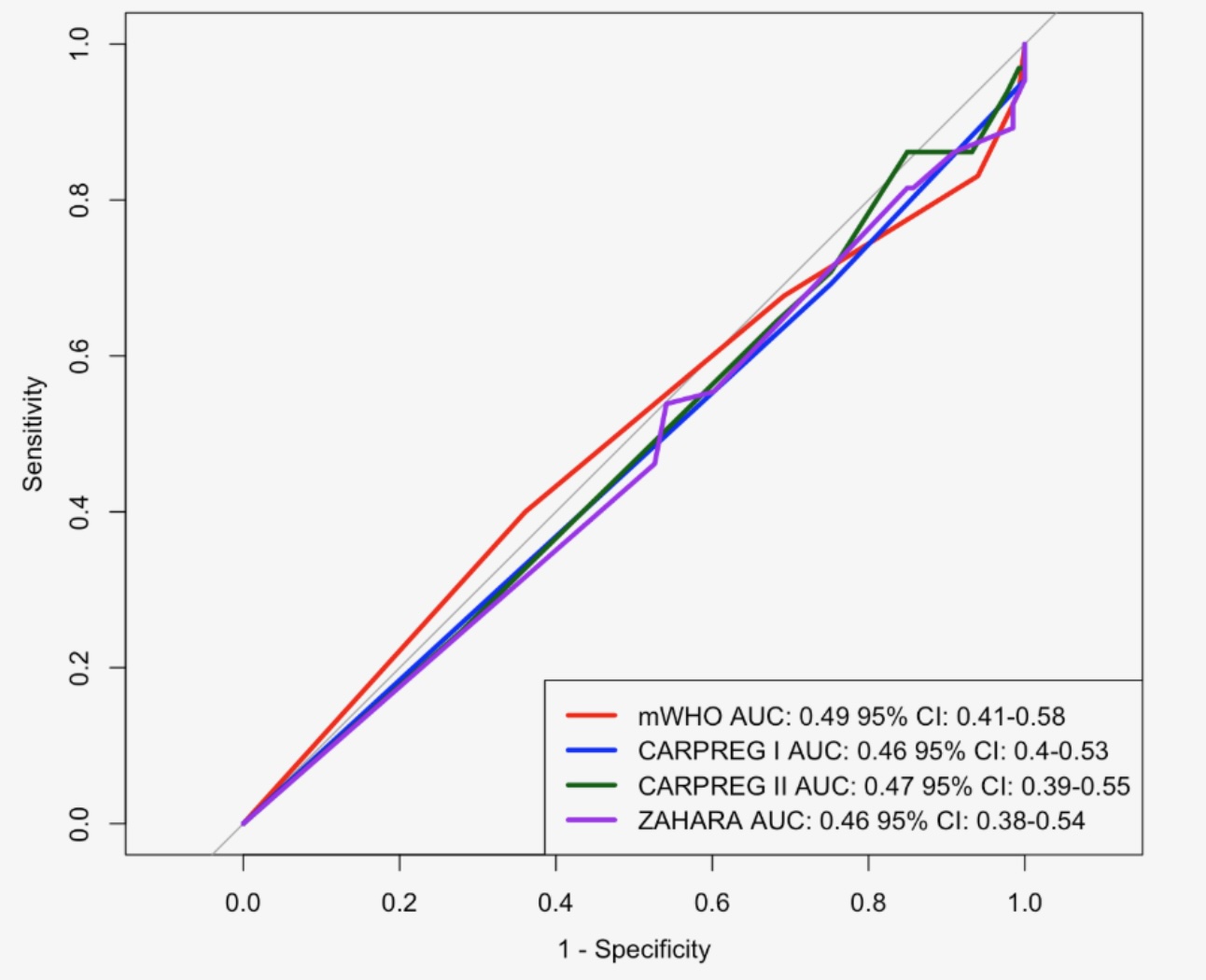
Background: Improved management of adult CHD has led to a growing number of patients reaching childbearing age. While the need for accurate risk assessment has increased, current tools to predict neonatal outcomes remain limited. Existing cardiac risk models were developed to predict maternal cardiovascular complications and have not been validated for neonatal outcomes. Objective: This study evaluated how current cardiac risk stratification tools predict neonatal outcomes in adult pregnant women with CHD and examined individual risk predictors for adverse neonatal outcomes. Design/Methods: A retrospective chart review was performed of 198 pregnancies among patients with CHD ≥18 years old receiving care at the MFM-Cardiology Joint Program at Montefiore Medical Center/Albert Einstein College of Medicine in the Bronx, NY from Jan 2015 to Dec 2024. Risk scores were calculated using the mWHO, ZAHARA, CARPREG I, and CARPREG II models. The primary outcome was predictive performance for neonatal complications using receiver operating characteristic (ROC) curve analysis, with comparison of event rate distribution per model via Fisher's exact test. Secondary analyses identified individual predictors of neonatal complications. Results: Of 198 pregnancies, 65 (32.8%) had neonatal complications antepartum or in the neonatal period. ROC analysis demonstrated poor discriminative ability with an area under the curve (AUC) ≈ 0.5 for all four models (Figure 1). Absolute rates of neonatal complications generally increased with higher maternal risk scores in all models, though few incremental changes reached statistical significance (Figure 2). Significant (p < 0.05) univariate risk predictors for neonatal complications included pulmonary hypertension/cyanosis/NYHA functional class >II, cardiac medication during pregnancy, high-risk valve disease/left heart obstruction, anticoagulation during pregnancy, and smoking during pregnancy (Table 1).
Conclusion(s): Existing cardiac risk tools showed limited ability to predict neonatal complications among pregnant women with CHD. Although higher maternal risk scores were generally associated with increased neonatal events, these relationships were largely nonsignificant, likely due to small sample sizes in higher risk groups. Findings suggest that tools developed for maternal cardiac risk may not adequately describe neonatal risk, reflecting insufficient inclusion of obstetric and behavioral factors influencing neonatal outcomes. Independent predictors identified here highlight the need for comprehensive tools to improve neonatal risk prediction and management for pregnancies complicated by CHD.
Figure 1. Receiver operating characteristic (ROC) curves of neonatal events for cardiovascular risk assessment models
Figure 2. Observed adverse neonatal events (%) for the cardiovascular risk assessment models mWHO, ZAHARA, CARPREG I, CARPREG II
Table 1. Univariate model for predicting neonatal outcomes in n=198 pregnancies from January 2015 to December 2024


.png)