311 - A Pilot Analysis of Patient Anthropometrics and Health Related Quality of Life for Enterally Autonomous Pediatric Patients Receiving Enteral Nutrition through an Immobilized Lipase Cartridge
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3300.311
Jason Soden, University of Colorado School of Medicine, Denver, CO, United States; Megan Aarnio-Peterson, Alcresta Therapeutics, Waltham, MA, United States; Justin Neal, PRO-spectus, Baldwinsville, NY, United States; Lynn B. Wilson, Alcresta Therapeutics, Lakeville, MA, United States; Michael M.. Yeh, Alcresta Therapeutics, Waltham, MA, United States; David Recker, Alcresta, Libertyville, IL, United States
Professor of Clinical Pediatrics University of Colorado School of Medicine Denver, Colorado, United States
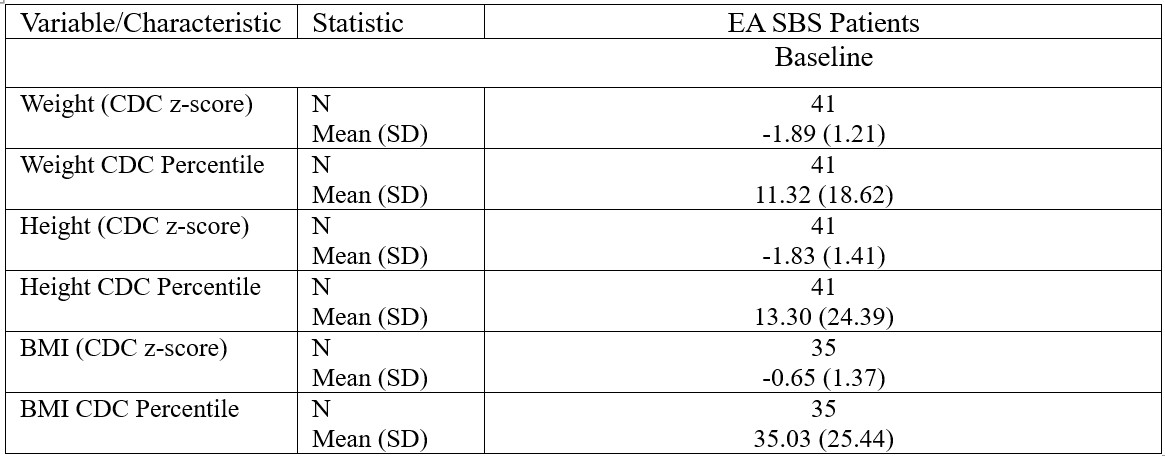
Background: Achieving enteral autonomy (EA) is a primary goal in the management of pediatric patients with short bowel syndrome (SBS) in order to avoid risks associated with parenteral nutrition administration. Despite achieving EA, patients may experience ongoing malabsorption due to altered intestinal anatomy leading to digestive symptoms that negatively impact quality of life and guarded nutritional status over time. Therefore, therapies intended to improve nutrient absorption may improve nutritional status and symptoms in patients with SBS. Objective: A porcine SBS model showed improved nutrient absorption by providing enteral nutrition through an immobilized lipase cartridge (ILC). These pre-clinical data suggest that integration of ILC with enteral nutrition may be of benefit in pediatric patients with SBS. Design/Methods: To assess this in clinical practice, a prospective direct-to-patient registry was launched in July 2024 to collect real-world data on pediatric SBS patients receiving enteral nutrition (EN) with RELiZORB (ILC). This initial analysis evaluates ILC efficacy in patients who have achieved enteral autonomy (EA), based on medical history, anthropometrics, HRQOL, and EN progression. Results: A total of 42 EN only SBS participants were enrolled as of July 31, 2025. Although these participants had achieved EA, their baseline anthropometrics at registry entry were still below normal growth expectations (Table 1). Following 3 and 6 months of ILC usage, EA participants gained weight at a greater rate as shown below by positive CDC z-scores, despite no concomitant increase in EN calories (Figure 1).
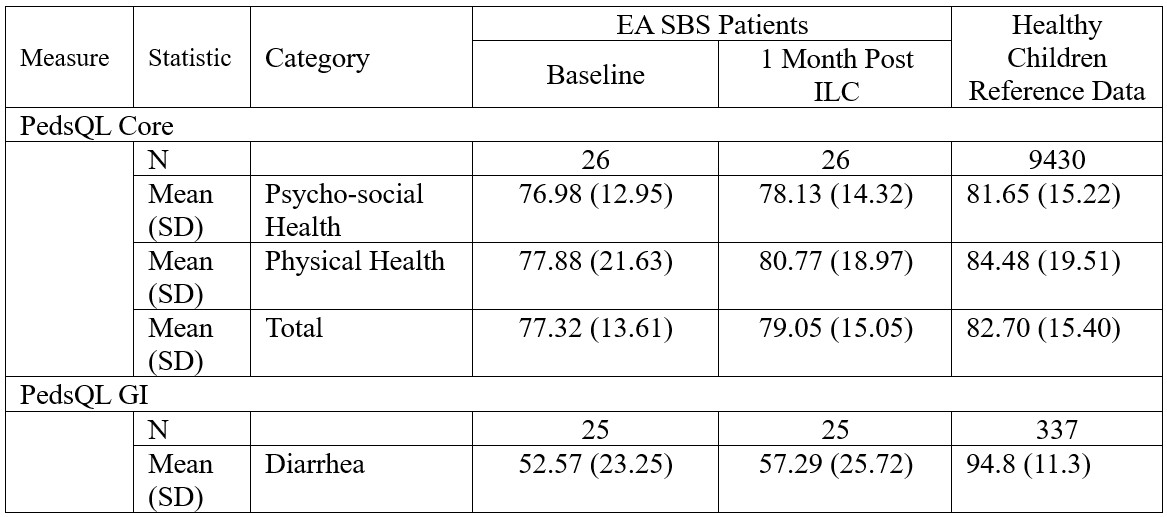
Mean PedsQL core and diarrhea GI (gastrointestinal) scores for EA SBS participants were lower at baseline compared to established standards (Table 2). Following one month of ILC usage, participants showed higher total PedsQL and PedsQL diarrhea GI scores. However, these increases were not greater than the minimal clinical important difference (MCID) for these instruments.
Conclusion(s): Encouraging preliminary findings from this limited subset suggest potential efficacy benefits in EA pediatric SBS participants using ILC. These initial anthropometric changes and HRQOL results highlight that SBS patients who have achieved EA continue to experience growth challenges and GI issues that may be improved through improving fat hydrolysis. Building on this pilot analysis, additional analyses with more participants are planned with results anticipated by April 2026.

.jpg)