576 - ARVIN - Augmented reality ventilation and intubation in neonates
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3557.576
Michael Wagner, Medical University of Vienna, Vienna, Wien, Austria; Carlotta Moira. Westphal, Free university Berlin, Berlin, Berlin, Germany; Robyn Dvorsky, Medical University of Vienna, Vienna, Wien, Austria; Charles C. Roehr, University of Bristol, Bristol, England, United Kingdom; Paula Vécsei, Medical University of Vienna, Wien, Wien, Austria
Prof Medical University of Vienna Vienna, Wien, Austria
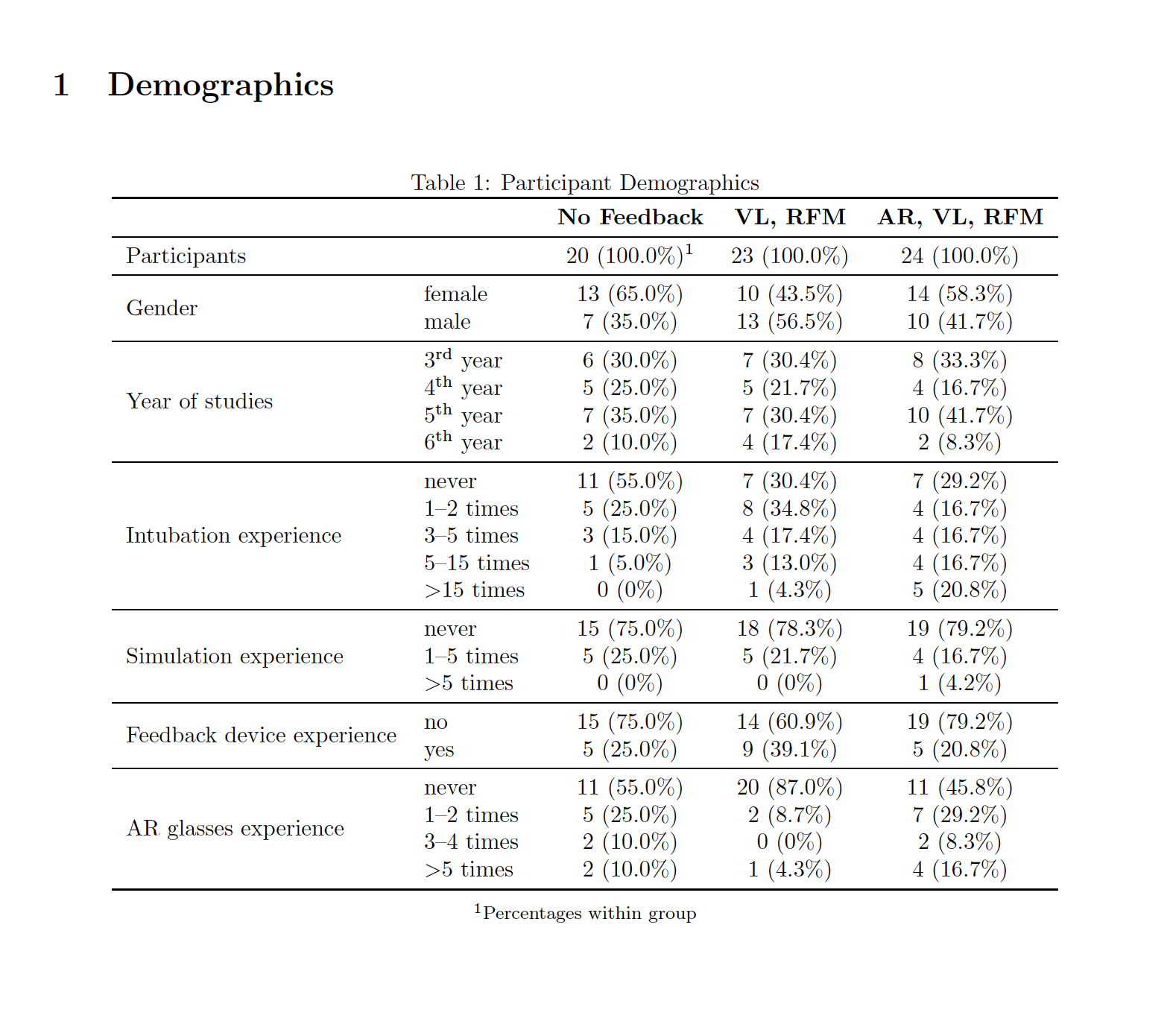
Background: Airway management during newborn resuscitation at birth is hampered by operator information overload, leading to variable performance. Respiratory function monitors (RFM) have been shown to improve the quality of manual ventilation. Video-Laryngoscopy (VL) has been touted to improve first-pass intubation success. However, integrating RFM data and video-signal in the stressful delivery room (DR) resuscitation scenario is immensely challenging. Human factors, especially distractibility, cause operator variations, potentially compromising outcome. Augmented reality (AR) glasses have been shown to improve performance by integrating monitoring signals from different sources within one visual field. Objective: We hypothesized that using AR for training airway management during newborn resuscitation limits operator distractibility and improves ventilation and intubation performance. Design/Methods: Randomized controlled simulation of DR resuscitation comparing 3 groups with different feedback access. Group 1 had no feedback, group 2 used RFM and VL, group 3 used AR, with RFM and VL monitors transmitted to the AR visual field. The scenario included mask ventilation of a term manikin, then intubation via VL. Outcome measures were mask leak, ventilation rate, tidal volume, intubation attempts, time to successful intubation, feasibility and usability of AR. Participants rated their experience in a post-study questionnaire. Results: We included 72 participants randomly allocated to three groups. Participant characteristics are in table 1. Reliable results came from 67. A few results are shown in table 2. Integration of RFM and VL monitoring via AR did not significantly improve ventilation performance compared to the conventional setting. Participants wearing AR had slightly less mask leak and better ventilation rates (p < 0.05). They needed fewer but longer intubation attempts. Over 70% reported AR use during resuscitation was feasible and usable.
Conclusion(s): The integration of RFM and VL signals in the visual field did not show significant improvement in mask ventilation but did for intubation. We speculate that the sample size may have been too low, as differences between groups 2 and 3 were not statistically significant. The lack of effect may reflect data variance, technical issues, novelty and limited practice.

 photo")
.png)
.jpg)
