Consultant Neonatologist Monash Children's Hospital, Melbourne Clayton, Melbourne, Victoria, Australia
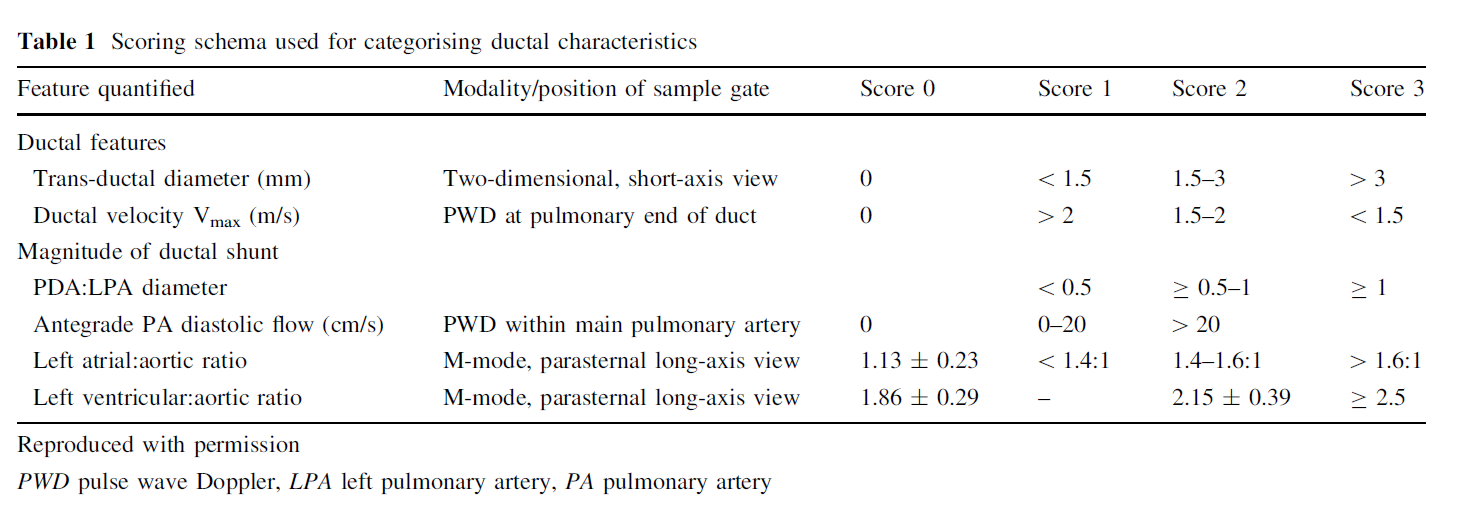
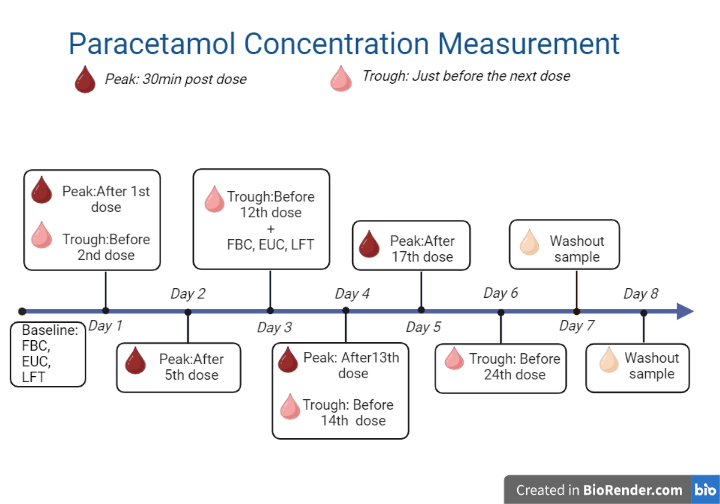
Background: Patent ductus arteriosus (PDA) remains a prevalent condition among preterm infants, often necessitating pharmacologic intervention to promote closure and prevent associated morbidities. Acetaminophen has emerged as a potential alternative to cyclooxygenase inhibitors but the relationship between its plasma concentration and therapeutic efficacy is not well established. Objective: This prospective clinical study investigated whether acetaminophen plasma levels are associated with successful PDA closure in preterm neonates born at < 28 weeks gestational age(GA). Design/Methods: Preterm neonates were evaluated by echocardiography (ECHO) for PDA and were treated if the ductal shunt was hemodynamically significant using PDA scoring schema Figure1. The dosage for acetaminophen was 15 mg/kg every 6 h for three days (first course). A second course of acetaminophen for three days was given if there was ductal patency. Baseline creatinine, liver function test and platelet count were checked before the commencement of each course of acetaminophen therapy. Serum acetaminophen levels were checked at various time points during each acetaminophen course as shown in the Figure 2. The primary outcome was association of PDA closure to plasma acetaminophen levels. Successful treatment was defined a priori as complete closure or ≥50% reduction in the composite PDA score. Results: Thirty -two preterm infants with a median(IQR) GA of 24 weeks (24, 26) and birth weight of 645 g (576, 756) received acetaminophen therapy at a median(IQR) postnatal age of 4.5 days (3, 8.5). Acetaminophen treatment was successful in 12 /32 (37.5%) neonates. Median (IQR) acetaminophen concentrations (μmol/L) did not differ significantly between neonates with or without PDA closure [164 (119, 203) vs. 187 (105, 251); P=0.47], Figure3. Neonates with PDA open after treatment were of significantly lower GA (median (IQR)) 24 (23, 24) compared to neonates with PDA closure 25 (25, 26) and had significantly lower antenatal steroid exposure 8/18 (44%) vs. 10/12 (83%), however their birth weights were similar. In adjusted analyses, acetaminophen plasma levels were not independently associated with PDA closure (adjusted OR (95% CI) 1.00 (0.98, 1.01); P=0.95). No serious adverse events related to acetaminophen were noted during the study period.
Conclusion(s): These findings suggest that plasma acetaminophen levels may not be a reliable predictor of successful PDA treatment. Further research is needed to elucidate the mechanisms underlying acetaminophen's therapeutic effects and to identify clinical or biochemical markers that better predict response.
Figure2. Timeline of blood sample collection for Acetaminophen level measurement

.png)