TOP 67 - The Relationship between Human Milk Fortifier and Metabolic Acidosis among Preterm Neonates
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4771.TOP 67
Madhur Pantola, Mount Sinai Hospital, Toronto, ON, Toronto, ON, Canada; ASHRAF KHARRAT, Sinai Health System, Toronto, ON, Canada; Kirsten Kotsopoulos, Sinai Health System, Toronto, ON, Canada; Noura Hersh, Mount Sinai, Toronto, ON, Canada; Amrita Sandhu, Mount Sinai Hospital, Brampton, ON, Canada; Emma Liu, Mount Sinai Hospital, Toronto, ON, Canada; Prakesh S. Shah, Mount Sinai Hospital, Toronto, ON, Canada
Neonatal Perinatal Fellow Mount Sinai Hospital, Toronto, ON Toronto, Ontario, Canada
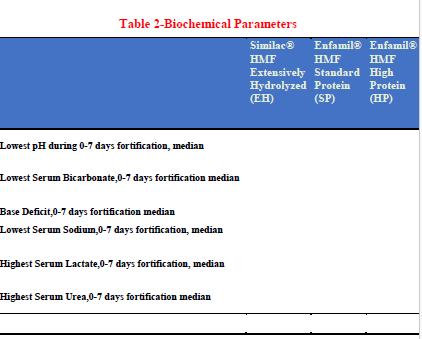
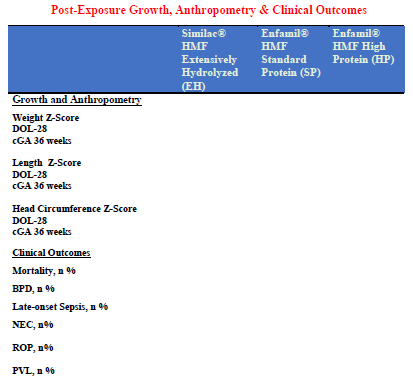
Background: Expressed breast milk or donor human milk are the preferred nutritional sources for preterm infants; however, their native protein and mineral content may not meet elevated nutritional needs. Human milk fortifiers (HMFs) are added to address these deficits, but available products differ in macronutrient composition and mineral content. Emerging evidence links certain fortifiers, especially acidified or high-protein formulations, to metabolic acidosis, defined by pH < 7.35, bicarbonate < 18 mmol/L, or base excess < −4 mEq/L. Preterm infants, with immature renal and buffering capacity, are vulnerable to acid–base imbalance, which may impair feeding tolerance, growth, and respiratory stability, and prolong NICU stay. Despite these concerns, comparative data on the biochemical impact of different HMFs remain limited. Objective: The primary objective is to compare the incidence of new-onset metabolic acidosis within 7 days of starting human milk fortification with Similac® HMF Extensively Hydrolyzed (EH), Enfamil® HMF Standard Protein (SP), and Enfamil® HMF High Protein (HP) in preterm infants born < 32 weeks gestation. Secondary objectives are: (1) to compare the duration and severity of metabolic acidosis (lowest pH, bicarbonate, and base deficit); (2) to evaluate associated biochemical changes (electrolytes, lactate, glucose, urea, and creatinine); and (3) to assess anthropometric outcomes. Design/Methods: A retrospective matched cohort study will be conducted in the tertiary NICU at Mount Sinai Hospital (Toronto). Eligible infants are < 32 weeks gestation, < 4 weeks old at fortifier initiation, and receiving mother’s or donor milk. Exclusions include major anomalies, inborn errors of metabolism, NEC ≥ stage II, and sepsis at fortification start. Fortifier use varied by period: EH (Jan 2021–Jun 2022), SP (Jul 2022–Dec 2023), and HP (Jan 2024–Jun 2025). Infants with at least one blood gas within 7 days of fortification will be included. Detailed biochemical, anthropometric, and illness severity data will be collected at baseline, within 7 days, and at NICU discharge. The HP group (4 g protein/100 kcal) will serve as the primary exposure cohort. Each HP infant will be matched 1:1:1 with one SP and one EH control by gestational age (± 1 week), birth weight (± 100 g), and sex. Assuming a 20% incidence of metabolic acidosis, a total of 219 infants (73 per group) will be required. REB approval has been obtained.

 photo")