Session: Neonatal General Trainee Ongoing Projects
TOP 59 - Intrahepatic Cholestasis of Pregnancy: Neonatal Considerations and Outcomes in An Ethnically High-Risk Population
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4763.TOP 59
Amrita Suresh, Icahn School of Medicine at Mount Sinai/Elmhurst, Elmhurst, NY, United States; Pushwinder Kaur, Icahn School of Medicine at Mount Sinai/Elmhurst, Newyork, NY, United States; marco nunez Ramos, Icahn School of Medicine at Mount Sinai, Rego Park, NY, United States; Uday P.. Patil, Icahn School of Medicine at Mount Sinai-NYC H+H/Elmhurst, Elmhurst, NY, United States
Pediatric Resident Physician Icahn School of Medicine at Mount Sinai/Elmhurst Elmhurst, New York, United States
Background: Intrahepatic cholestasis of pregnancy (ICP) is a common liver disease in pregnancy, presenting with pruritus and elevated serum bile acids in the late second or third trimester. Maternal ICP affects fetal and neonatal outcomes, including preterm birth, meconium at birth, and stillbirth. Ursodeoxycholic acid (UDCA) is the first-line treatment, but its impact on neonatal outcomes is unclear. ACOG and SMFM recommend management based on maternal total bile acid (TBA) levels. While ICP occurs in 0.3-0.5% of pregnancies in the U.S., rates are much higher (5-15%) in Hispanic and Asian populations, mainly cared for at our hospital. Data on neonatal outcomes in this ethnic population in the United States are scarce. Objective: To evaluate neonatal outcomes of maternal ICP under current guidelines in a high-risk population. The study also discusses the incidence of stillbirth, categorized by ICP severity. Design/Methods: In this IRB-approved study (Mount Sinai School of Medicine), a retrospective cohort of neonates born to mothers diagnosed with ICP at NYC H+H/Elmhurst Hospital between October 2020 and October 2025 is identified for an electronic medical record review (Epic systems) of both maternal and neonatal charts. Cases where the mother had a previous pregnancy with ICP or pre-existing liver disease are excluded. Statistical analyses will be conducted using SAS. The Mann-Whitney U test, Chi-Square test, and multivariate regression analyses will be used to investigate relationships between neonatal outcomes and the severity of maternal ICP. Data analysis is expected to be completed by December 31, 2025.
Preliminary
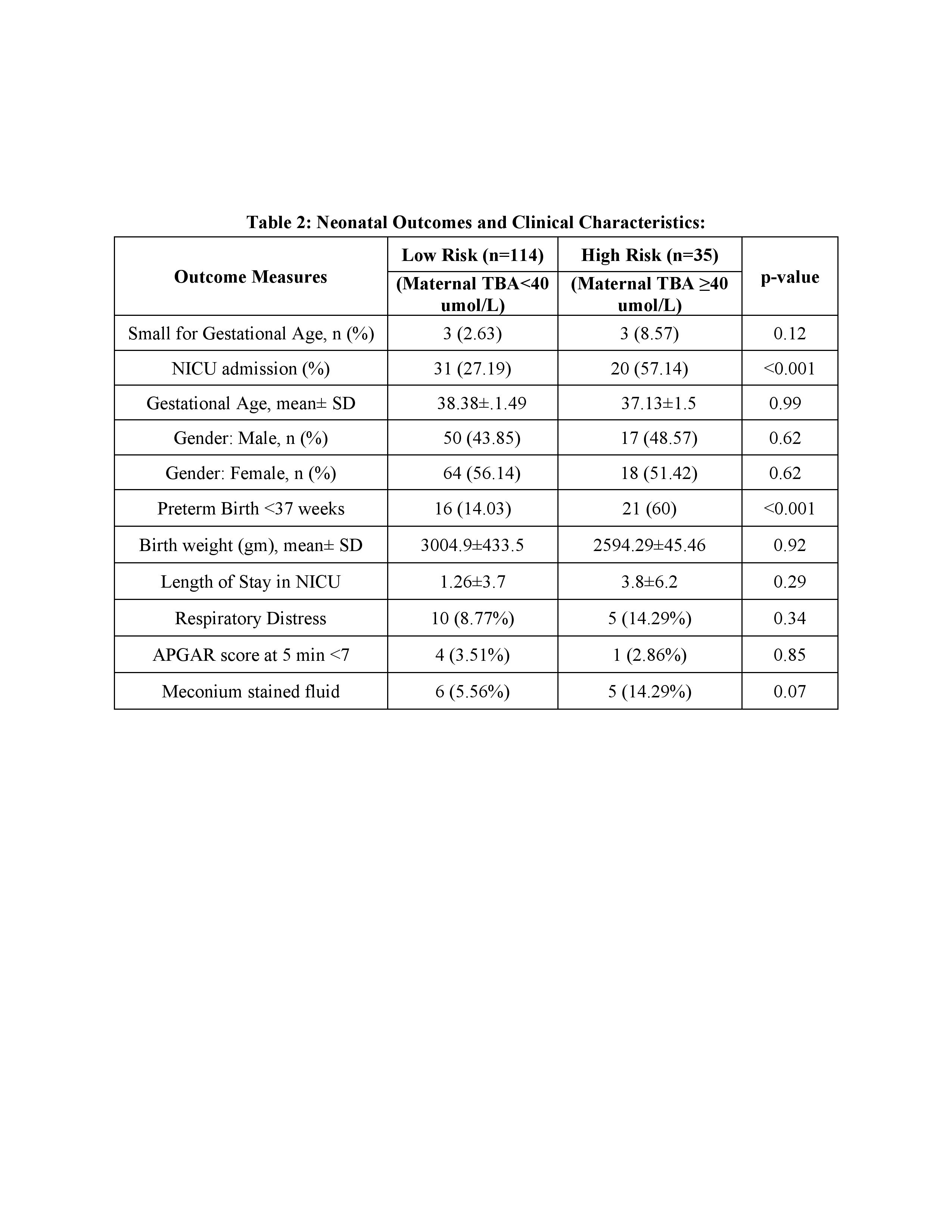
Results: A total of 478 neonates were identified with a maternal diagnosis of ICP during the study period. Of these, 162 charts were reviewed in a pilot data assessment. Thirteen charts were excluded based on the study's exclusion criteria. Charts were categorized into low-risk (LR) (TBA < 40 umol/L) and moderate-to-high risk (MHR) (TBA ≥ 40 umol/L) groups. Maternal demographic and clinical characteristics are shown in Table 1. Both groups had similar characteristics except for body mass index. The pruritis rate and UDCA utilization are very high in our population. The neonatal outcomes show significantly higher NICU admissions (p < 0.001), preterm births (p < 0.002), and a trend toward significance for meconium-stained amniotic fluid at birth (p=0.07) (Table 2). As we review the remaining data, we expect more statistically significant associations to emerge. No stillbirths or neonatal deaths were noted at the time of this analysis.
Table 1: Maternal Demographic and Baseline Clinical Characteristics
Table 2: Neonatal Outcomes and Clinical Characteristics:

.jpg "Amrita Suresh, MD (she/her/hers) photo")
.jpg)