410 - From Habit to Stewardship: Assessing the Appropriateness of Azithromycin Use in Pediatric Acute Care.
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4401.410
Shayla Eaklor, Southern Illinois University School of Medicine, Springfield, IL, United States; Ezzeldin Saleh, Southern Illinois University School of Medicine, SPRINGFIELD, IL, United States; Myto Duong, Southern Illinois University School of Medicine, Springfield, IL, United States; Marcela Rodriguez, Southern Illinois University School of Medicine, Springfield, IL, United States; Kristin Delfino, Southern Illinois University School of Medicine, Springfield, IL, United States; Sharon Kim, Southern Illinois University School of Medicine, Springfield, IL, United States; Peyton Keller, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States; subhash chaudhary, Southern Illinois University School of Medicine, Springfield, IL, United States
Resident Southern Illinois University School of Medicine Springfield, Illinois, United States
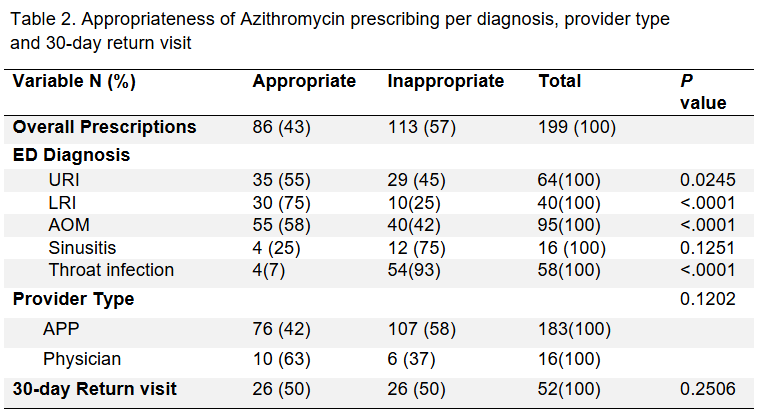
Background: Azithromycin is commonly prescribed to children with upper and lower respiratory tract infections despite clinical practice guidelines advising against its use for conditions such as acute otitis media, nonspecific upper respiratory infection (URI), sinusitis or acute pharyngitis, except in cases of severe beta-lactam allergy. Despite these recommendations, inappropriate prescription of azithromycin in emergency departments (ED) and urgent care (UC) settings continues and leads to adverse drug effects, antibiotic resistance, and increased healthcare costs. Objective: We aimed to investigate azithromycin prescribing patterns and appropriateness for children seen in ED and UC in our community and estimate rate of 30-day ED/UC return visits. Design/Methods: We performed a retrospective chart review, of pediatric patients prescribed azithromycin in local EDs and UCs between December 2023 and May 2024. Data collected included patient demographics, diagnoses, allergy history, azithromycin prescription, provider type, and 30-day return visits. Inappropriate prescribing defined as deviation from guidelines was assessed. Descriptive statistics and Chi-square analyses were performed using SAS version 9.4. Results: Among 199 pediatric patients evaluated, 87% were seen in UC and 13% in the ED. The mean age was 6.4 years, with 58% male and 80% white. Most common final diagnoses were acute otitis media (48%), URI (32%), and pharyngitis (29%). Reported allergies to penicillin and cephalosporins were 65% and 17%, respectively. Overall, 57% of azithromycin prescriptions were inappropriate, most commonly for pharyngitis (93%) and significantly associated with URI, lower respiratory infection (LRI), ear problems, and pharyngitis (p < 0.05). The 30-day return visit rate was 26% but was not significantly associated with inappropriate antibiotic use (p=0.25). Advance Practice Providers (APPs) had high prescribing rates of azithromycin (92%) Their prescribing represents 95% (107/113) of inappropriate azithromycin use. There were only 16 prescriptions by physicians of which 5% (6/113) were inappropriate which was not statistically significant.
Conclusion(s): In our community ED and urgent care settings, azithromycin is frequently and inappropriately prescribed, particularly for URIs and pharyngitis. APPs contributed to the majority of inappropriate prescribing. Targeted QI strategies, including provider and patients' education, automated decision-making and guideline dissemination, are necessary to optimize azithromycin prescribing practices.
Table 1. Characteristics of the study participants
Table 2. Appropriateness of Azithromycin prescribing per diagnosis, provider type and 30-day return visit

 photo")
.png)