629 - Preliminary inter-rater reliability and validity of the Neonatal Withdrawal Assessment Scale (NWAS) in preterm and critically ill infants with opioid withdrawal.
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4615.629
Ana Herning, Boston University School of Medicine, Boston, MA, United States; Cheryl L. Cheryl Slater, boston medical center, WILMINGTON, MA, United States; Rodica M. Turcu, Harvard Medical School, Boston, MA, United States; Carolyn A. Bleiler, Massachusetts General Hospital, Boston, MA, United States; Javed Mannan, UMASS Memorial Medical center, Worcester, MA, United States; Elisha Wachman, Boston Medical Center, Newton, MA, United States
Medical Student Boston University School of Medicine Boston, Massachusetts, United States
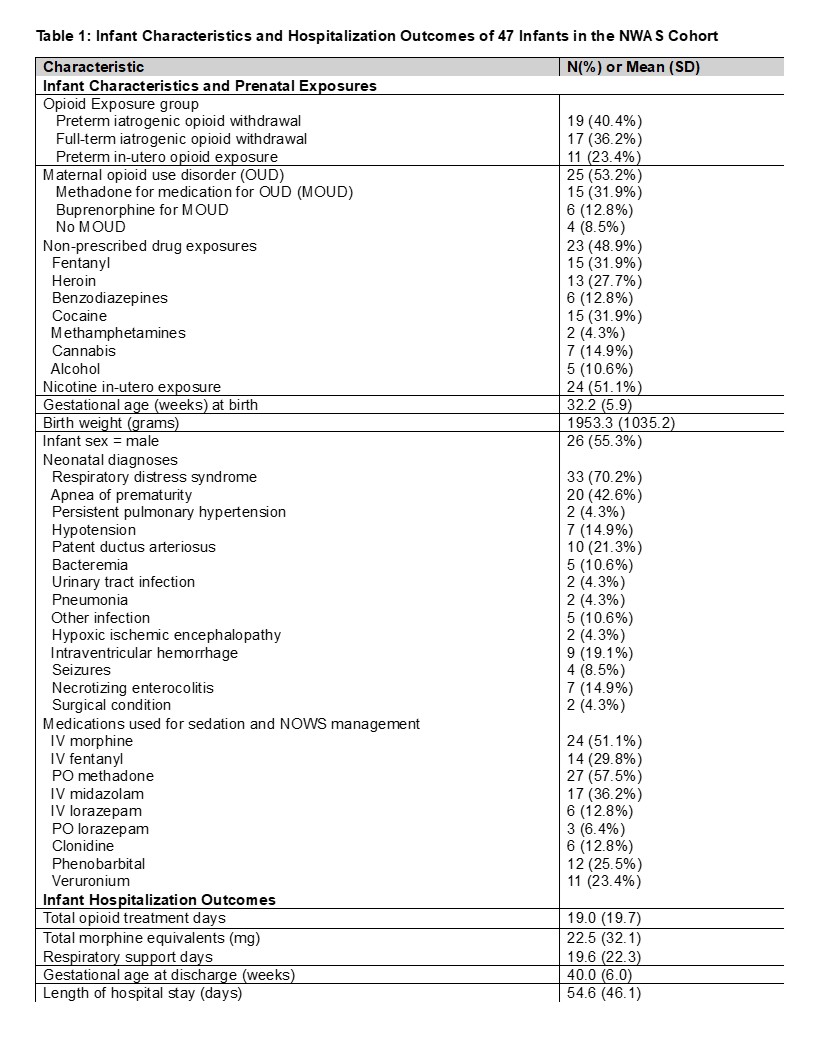
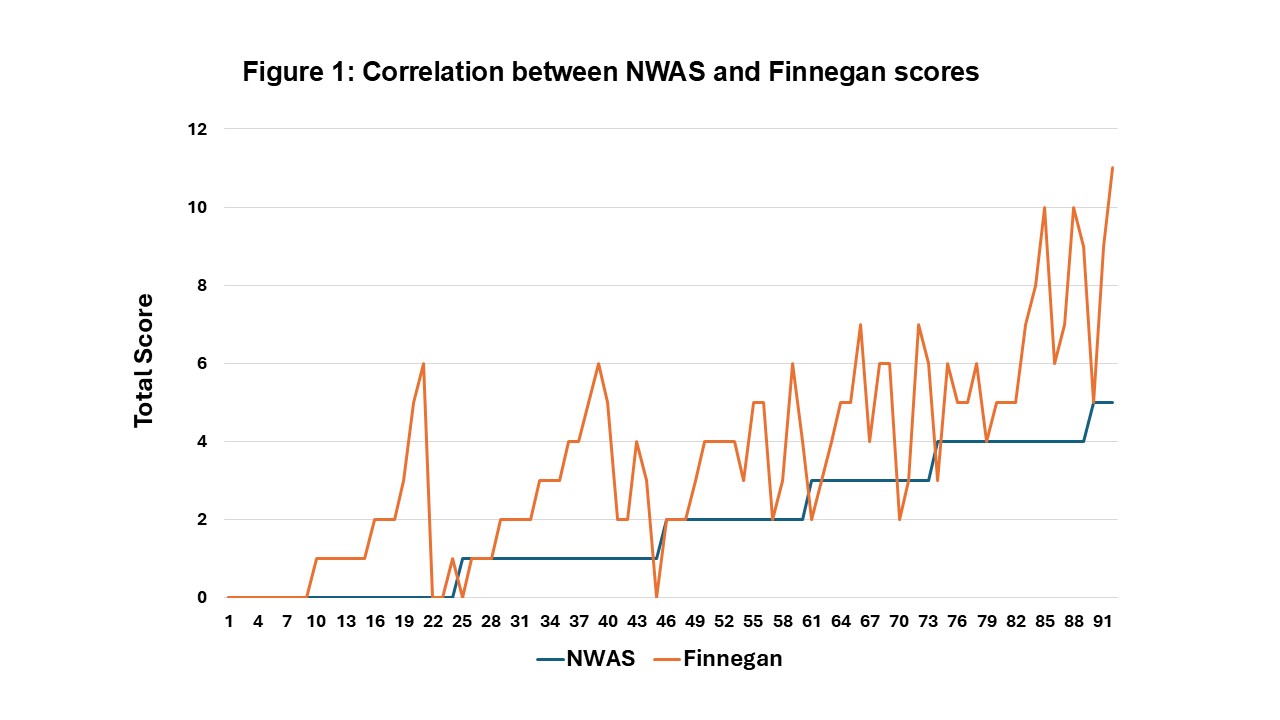
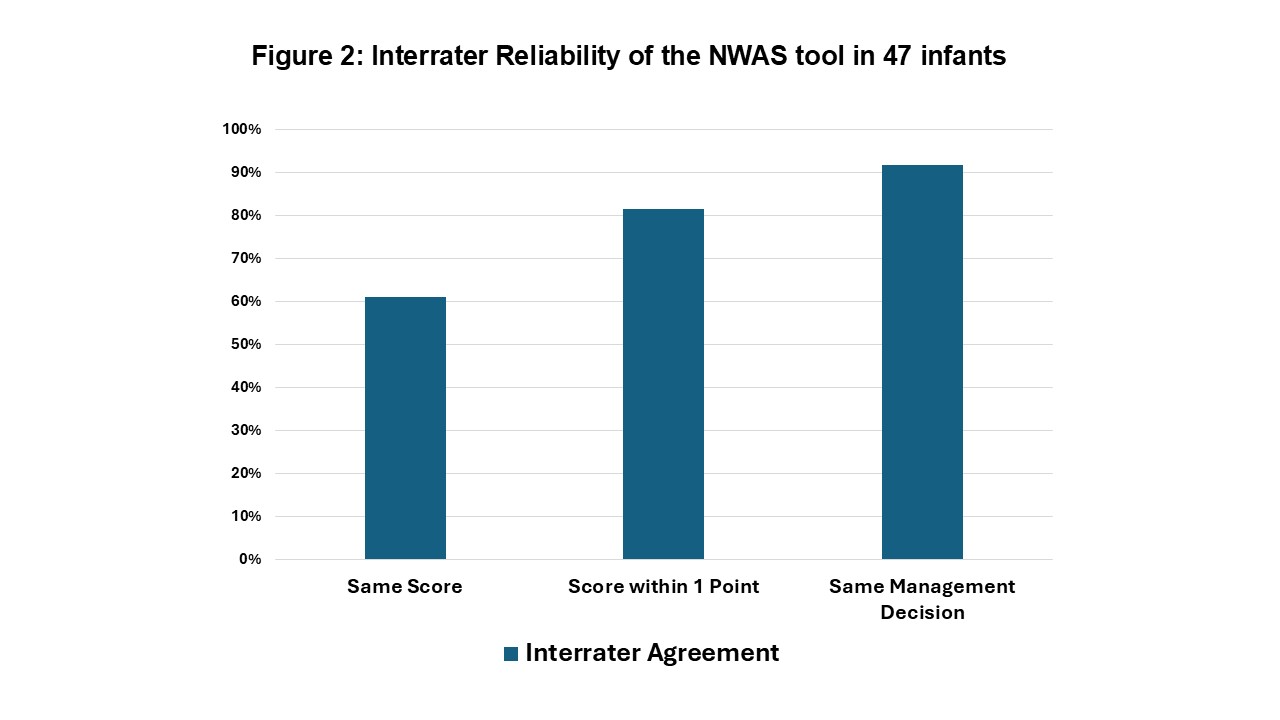
Background: Neonatal opioid withdrawal syndrome (NOWS) due to in-utero and/or iatrogenic opioid exposure has become a significant public health concern. Given its highly variable presentation and clinical outcomes, a standardized tool is integral in determining disease severity, assessing the need for pharmacologic intervention, and guiding medication management. Existing scoring systems include the Finnegan and Eat Sleep Console (ESC) tools; however, no standardized tool currently exists to evaluate NOW in premature or critically ill infants. Objective: To evaluate the reliability and validity of the newly proposed Neonatal Withdrawal Assessment Scale (NWAS) tool compared to the currently accepted Finnegan tool. Design/Methods: In a two-center study, preterm infants with in-utero opioid exposure born < 34 weeks of gestation or critically ill infants of any gestational age (GA) diagnosed with NOWS were scored based on the presence and severity of withdrawal symptoms using the NWAS tool by a bedside provider at the same time as a blinded gold standard rater. A subset of infants were dual scored with the Finnegan tool. Interrater reliability (IRR) was determined, and correlation between NWAS and Finnegan scores was calculated. Results: The NWAS cohort contained 47 infants (Table 1). The majority of infants had iatrogenic opioid exposure with 40.4% being preterm and 36.2% being full-term. The remaining 23.4% of infants were born preterm with in-utero opioid exposure. The mean GA of the cohort was 32.2 weeks (SD 5.9), and the mean birthweight was 1953.3 grams (SD 1035.2). Ninety-three simultaneous NWAS and Finnegan assessments were conducted across 15 infants. Using NWAS cut off scores >3 and Finnegan scores >8 for escalation of therapy, there was an 89% correlation between scores (Figure 1). For the 49 IRR incidences among 47 infants, the NWAS score was identical between raters in 61.2% of incidences and 81.6% of the time was within 1 point between raters (Figure 2). In 91.8% of incidences, the same management decision would be indicated between the bedside provider and gold standard rater based on the tool's cut-off scores.
Conclusion(s): Preliminary assessment of the NWAS tool demonstrated high IRR, as well as validity via strong correlation with the currently widely utilized Finnegan tool. Further examination of the association with management with the NWAS tool and clinical outcomes can inform future creation of evidence-based guidelines for the treatment of NOWS in premature and critically ill infants.
Infant Characteristics and Hospitalization Outcomes of 47 Infants in the NWAS Cohort
Correlation between NWAS and Finnegan Scores
Interrater Reliability of the NWAS tool in 47 Infants