313 - Timolol for Treatment and Prevention of Retinopathy of Prematurity
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4307.313
muppala Prasanth raju, Baylor Scott White McLane Children's Medical Center, Temple, TX, United States; Ashleigh Aubin, Baylor Scott White McLane Children's Medical Center, Temple, TX, United States; Niraj Vora, Baylor Scott White McLane Children's Medical Center, Leander, TX, United States; Venkata Raju, Baylor Scott White McLane Children's Medical Center, Temple, TX, United States; Vinayak Govande, Baylor Scott White McLane Children's Medical Center, Temple, TX, United States; Ram R.. Kalagiri, Baylor Scott White McLane Children's Medical Center, Temple, TX, United States; madhava (. Beeram, Baylor Scott and White Health, Temple, TX, United States; Ashith Shetty, Baylor Scott White McLane Children's Medical Center, Temple, TX, United States; Kushi Shetty, University of Texas at Austin, Austin, TX, United States; raza Bajwa, Baylor Scott and White, Temple, TX, United States
Fellow Baylor Scott White McLane Children's Medical Center Temple, Texas, United States
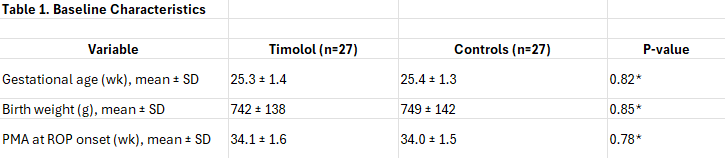
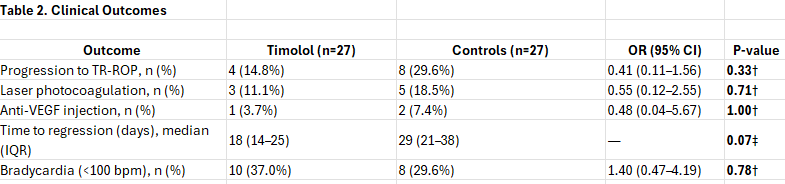
Background: Retinopathy of prematurity (ROP) is a vasoproliferative disorder affecting preterm infants and a major cause of preventable childhood blindness worldwide. Laser photocoagulation and anti-vascular endothelial growth factor (anti-VEGF) injections are established treatments for severe disease. Topical timolol, a non-selective beta-adrenergic blocker, may attenuate retinal neovascularization by reducing vascular endothelial growth factor (VEGF) expression and intraocular pressure. Objective: To assess the efficacy and safety of topical timolol in preventing progression to treatment-requiring ROP (TR-ROP; defined as Type 1 ROP or worse per Early Treatment for Retinopathy of Prematurity criteria) compared with matched untreated controls. Design/Methods: This retrospective 1:1 matched case-control study (2019-2025) included preterm infants diagnosed with Zone II, Stage 2 ROP with plus disease. Cases (n=27) received bilateral topical timolol 0.5% ophthalmic solution (1 drop twice daily) initiated at ROP diagnosis and continued until regression or progression to TR-ROP. Controls (n=27) received standard observation without timolol. Matching was performed on gestational age (GA; ±1 week), birth weight (BW; ±100 g). Primary outcome: progression to TR-ROP necessitating laser photocoagulation or anti-VEGF injection. Secondary outcomes: time from treatment initiation to regression and adverse events (e.g., bradycardia < 100 bpm, hypotension, or apnea). Results: Progression to TR-ROP occurred in 4/27 (14.8%) timolol-treated infants versus 8/27 (29.6%) controls (odds ratio [OR] 0.41, 95% confidence interval [CI] 0.11-1.56; p=0.33). Laser photocoagulation was required in 3/27 (11.1%) treated versus 5/27 (18.5%) controls (OR 0.55, 95% CI 0.12-2.55; p=0.71). Anti-VEGF injection was needed in 1/27 (3.7%) treated versus 2/27 (7.4%) controls (p=1.00). Median time to ROP regression was 18 days (interquartile range [IQR] 14-25) in the timolol group compared with 29 days (IQR 21-38) in controls (p=0.07, Wilcoxon rank-sum test). Bradycardia occurred in 10/27 (37%) timolol infants (both transient, resolving without intervention) versus 8/27 controls (p=0.78).
Conclusion(s): In this matched cohort, adjunctive topical timolol 0.5% was associated with numerically lower rates of progression to TR-ROP and laser therapy requirements, and a shorter median time to regression, though differences did not reach statistical significance. Transient bradycardia was more in the treated infants. Larger prospective randomized controlled trials are needed to confirm efficacy and establish clinical utility.