432 - Targeted Improvements of a Food Insecurity Screening Program in a Pediatric Emergency Department
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4423.432
Madeline E. Winn, Medical College of Wisconsin, Milwaukee, WI, United States; Michael L. Levas, MCW, CIC, Project Ujima, Pewaukee, WI, 53072, WI, United States; Ashley SERVI, Children's Hospital of Wisconsin, Milwaukee, WI, United States
Pediatric Emergency Medicine Physician Assistant Medical College of Wisconsin Milwaukee, Wisconsin, United States
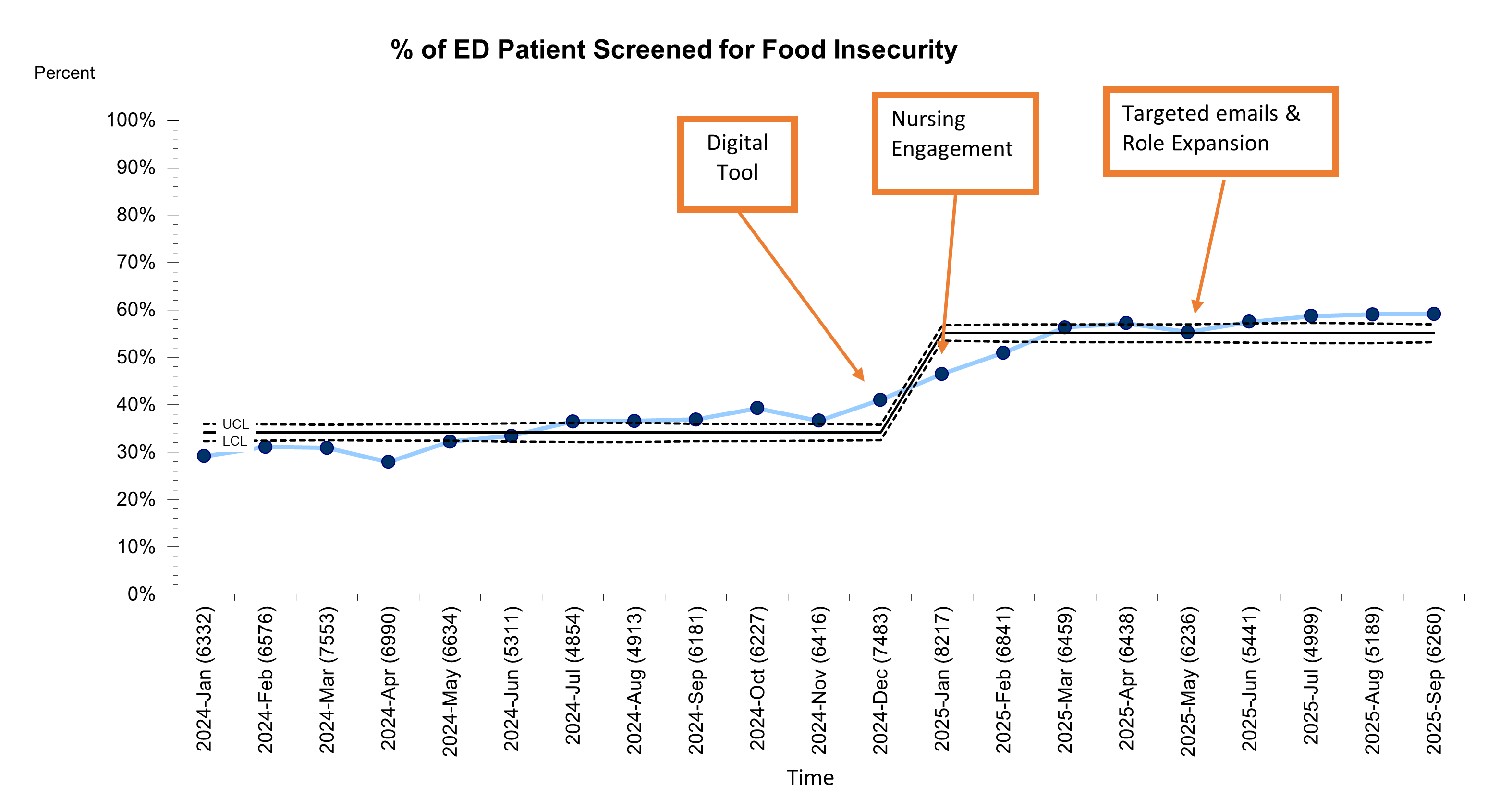
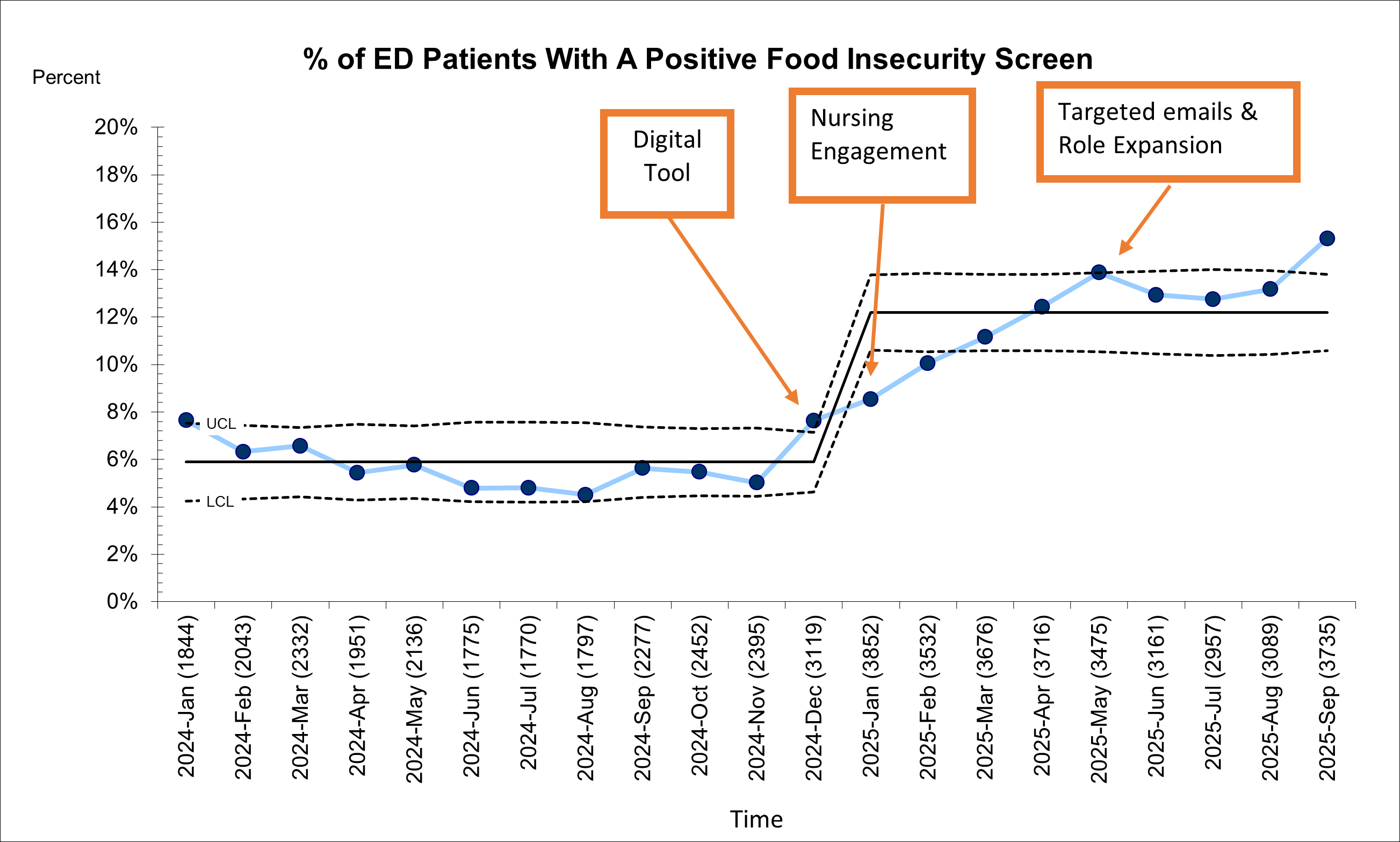
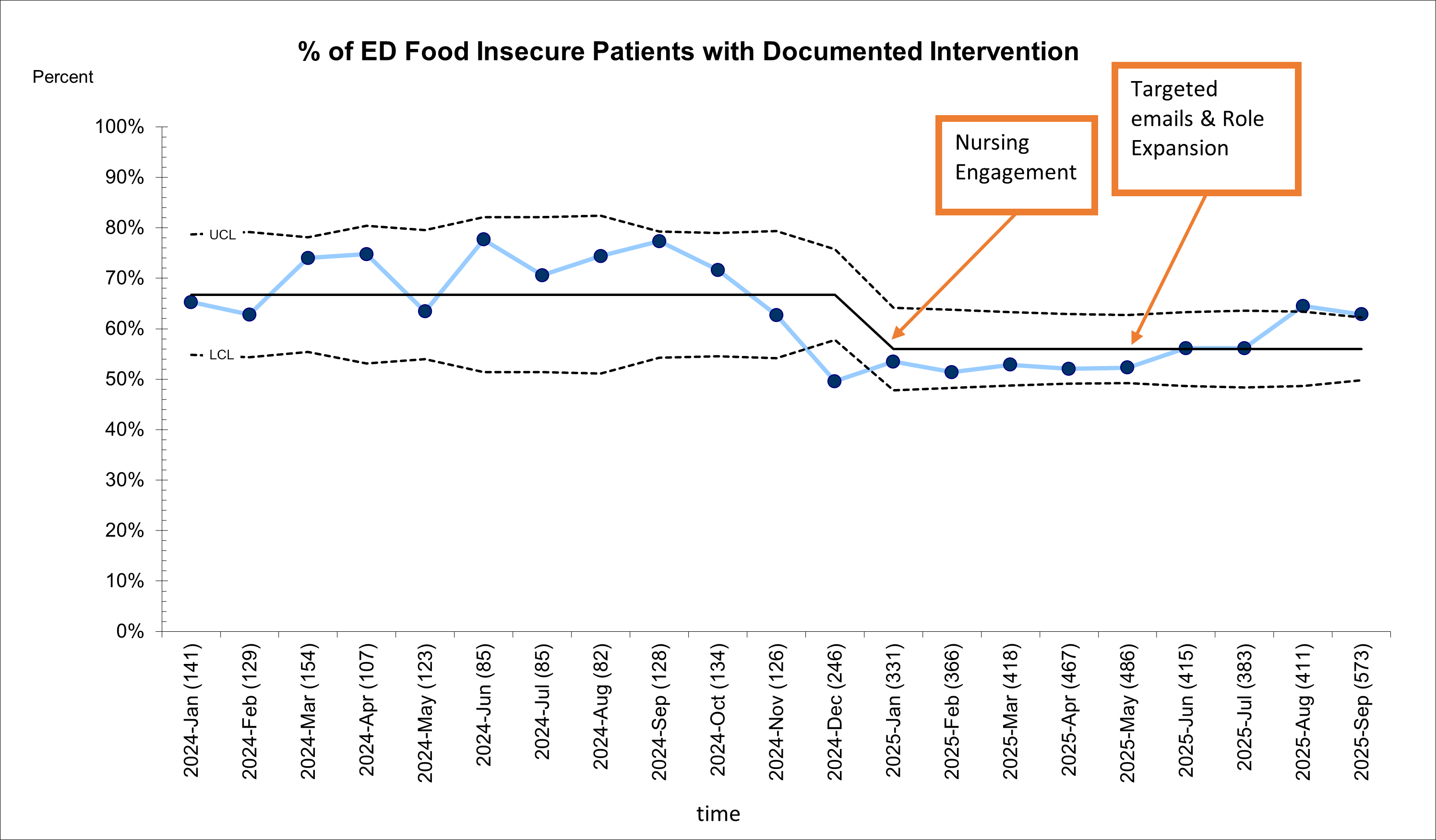
Background: Food insecurity (FI) affects more than 25% of children in Milwaukee County, placing them at increased risk for adverse health outcomes. FI is associated with elevated risks of multiple health conditions-including asthma, depression, developmental delay, and obesity. FI is also linked to disparities in healthcare utilization, including increased emergency department (ED) use and delayed or foregone preventive care. Our institution implemented a FI screening program in the pediatric ED. Utilizing a validated screening questionnaire, the program screens caregivers and provides resources. Screens completed via iPad app or verbally are tracked within the electronic health record (EHR). An identified need triggers ED staff to provide a food gift card with attached resources. Since its inception, screening rates varied between 6% and >70% with an average of 40%. This variability was the result of ineffective screening tools, absence of EHR decision support, and lack of clear role responsibility. Objective: Improve FI screening rates from 40% to 60% between 1/2025 and 9/2025. Design/Methods: Interventions were tested using plan-do-study-act cycles (PDSA) and included introduction of a digital screening tool, engagement with nurse leadership, expansion of roles involved in screening, and targeted follow up emails to staff. Key drivers included properly working digital devices and adequate staffing. Process measure was the number of screens completed by digital tool. The outcome measure was the number of patients screened for FI. Additional measure includes FI families that had a documented intervention. Results: Screening rates improved from pre-PDSA cycle rates of 40% to 55%. Screening modality has shifted with 43% of questions asked digitally compared to an average of 3% prior to interventions. FI rates also increased with a baseline rate of 6% and post PDSA cycle rate of 12.2%. Pre intervention documentation of resource averaged 67% with post PDSA cycle averaging 56%.
Conclusion(s): Digital tools, engagement with nurse leadership, expansion of roles involved in screening, and targeted follow up emails to staff all contributed to an increase in FI screening. Introduction of a digital tool and increase in digital tool use was associated with an increase in FI rates. However, role expansion decreased documentation of intervention in the EHR as limited roles have access to complete the documentation. These targeted interventions created a meaningful increase in percentage of patients screened for FI.
% of Ed Patients Screened for Food Insecurity
% of ED Patients With A Positive Food Insecurity Screen
% of ED Food Insecure Patients with Documented Intervention

 Credit")
 photo")