546 - Examining social determinants of health and the incidence of acute kidney injury in children
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4534.546
Anisha Kesarwani, Lucile Packard Children's Hospital Stanford, South San Francisco, CA, United States; Shina Menon, Stanford University School of Medicine, Palo Alto, CA, United States
Fellow Lucile Packard Children's Hospital Stanford South San Francisco, California, United States
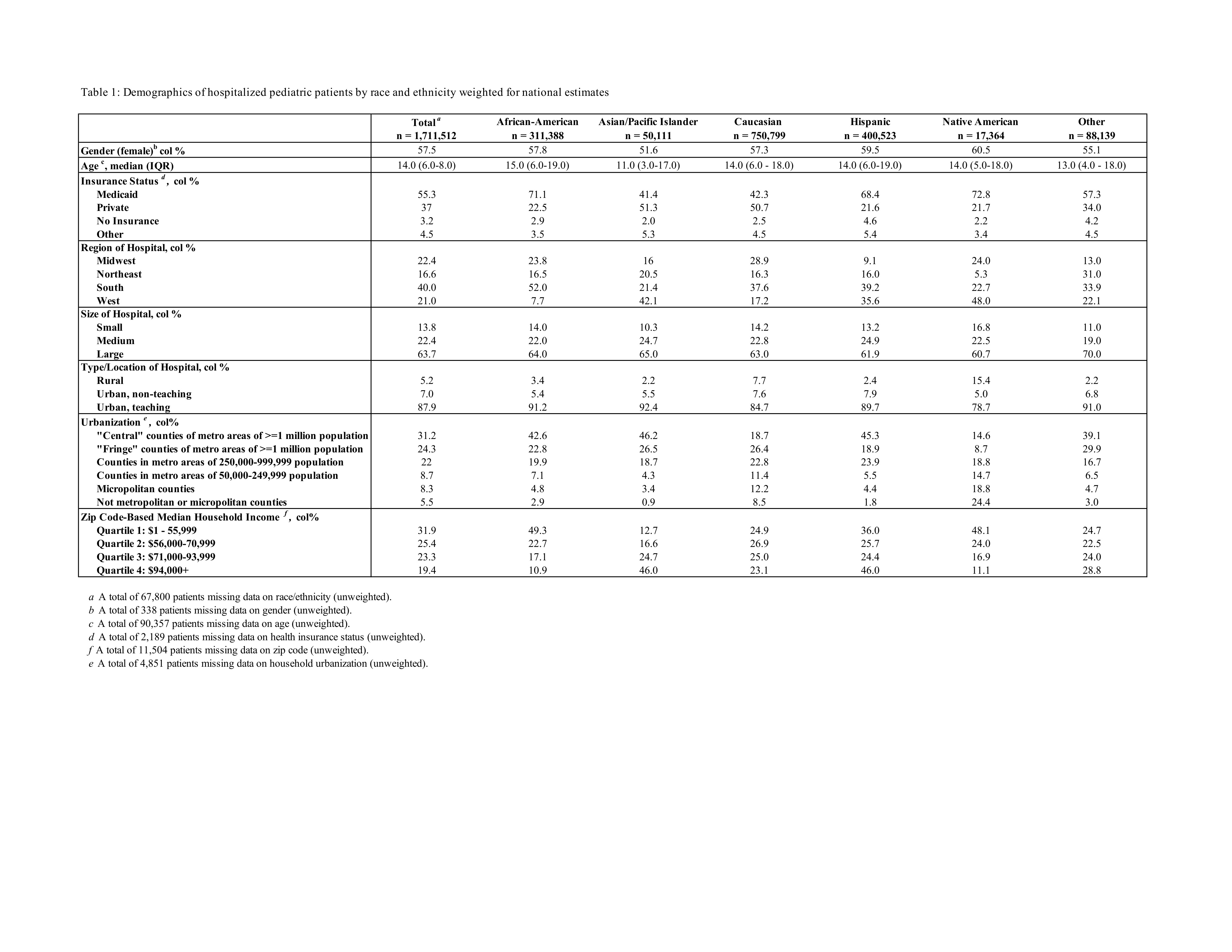
Background: Acute kidney injury (AKI) is common in hospitalized children. It is associated with increased morbidity and mortality in the short term, and higher risk of chronic kidney disease and hypertension in the long term. A prior analysis of > 1.6 million pediatric hospitalizations by Bjornstad, et al showed differences in race/ethnicity and insurance status in the incidence of AKI. We aimed to study the change in these data over the past decade. Objective: To quantify the national incidence of inpatient pediatric AKI in 2022 and measure absolute disparities of various socioeconomic factors.To contrast 2022 estimates with prior KID-2012 findings to assess changes in overall incidence and the pattern/size of disparities. Design/Methods: Secondary analyses of the 2022 Kids' Inpatient Database (KID) from the Agency for Healthcare Research and Quality. KID is a nationally representative sample of pediatric discharges throughout the USA. AKI was identified using ICD-10-CM N17.x. Survey design features (strata, cluster, weights) were applied to obtain national estimates. We calculated weighted AKI risks per 1,000 hospitalizations and univariate risk differences (RDs) versus prespecified references (White race, private insurance, zip-code median household income in the 3rd quartile, female sex, age 1-5 years, and large central metropolitan residence). Results: Among a total of 1,711,512 weighted pediatric discharges from ages 1-20 years, AKI occurred in 58,655, for an overall risk of 34.3/1000 discharges (Table 1). AKI risk was higher among boys (RD 20.5, 95% confidence interval (CI) 19.2-21.9, p< 0.0001) and increased steadily with age (all p< 0.0001). On univariate analyses, African-American children had higher risk of AKI compared with Caucasian children (RD 12, 95% CI 9.9-14.1; p< 0.0001) (Table 2). Hispanic children had lower risk (RD -4.1; 95% CI −6.2 to −1.9; p< 0.001). Compared with privately insured children, risk was modestly lower for Medicaid (RD -1.2, 95% CI -2.4-0.0; p=0.0498) but higher for uninsured (RD 10, 95% CI 6.6-13.4, p< 0.0001). Area-level zip income and urban-rural residence was not associated with AKI risk.
Conclusion(s): Pediatric AKI affected ~3.4% of U.S. hospitalizations in 2022 and remains unevenly distributed, with the greatest absolute burden among African-American and uninsured children. Compared with the KID-2012 era, national AKI incidence appears higher, underscoring opportunities for targeted kidney-safety and equity interventions. Next, we plan to adjust the risk differences for comorbidities, insurance status, gender, age, and household urbanization.
Table 1: Demographics of hospitalized pediatric patients by race and ethnicity weighted for national estimates
Table 2: Univariate risk estimates for sociodemographic differences in pediatric AKI episodes

.jpg)
