96 - Improving HPV Vaccination Rates in a Primary Care System
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4094.96
Corinna J. Rea, Boston Children's Hospital, Medfield, MA, United States; Eli Sprecher, Harvard Medical School, Boston, MA, United States; Jessica Barese, Boston Children's Hospital, Plainville, MA, United States; Kasey M. Papineau, Boston Children's Hospital, Cumberland, RI, United States; Shannon Regan, Boston Children's Hospital, Boston, MA, United States; Wendell Jean, Boston Children's Hospital, Brookline, MA, United States; Alexandra Epee-Bounya, Boston Children's Hospital, Boston, MA, United States
Assistant Professor Boston Children's Hospital Boston, Massachusetts, United States
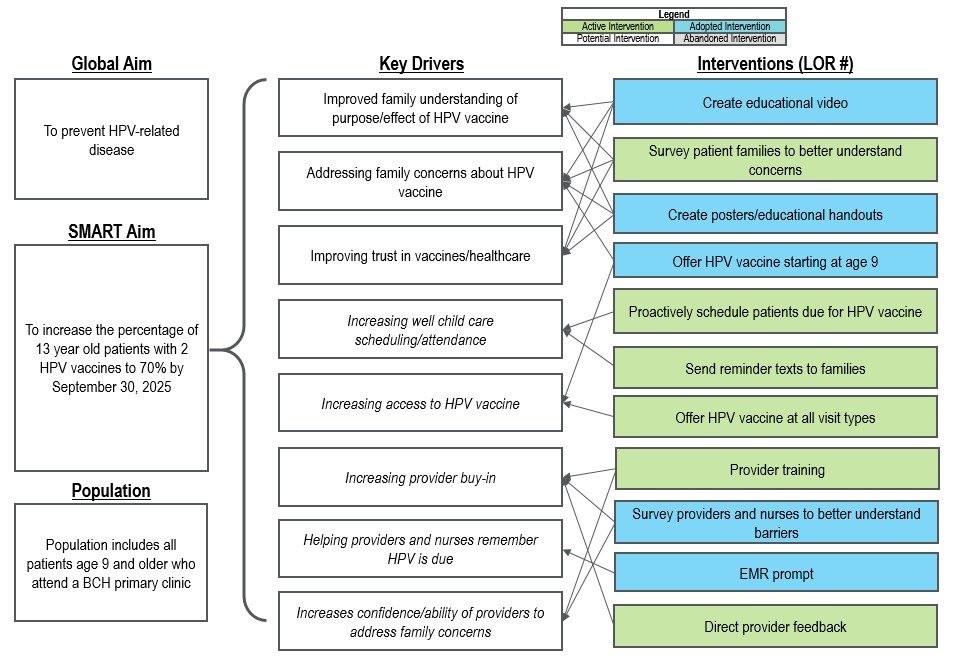
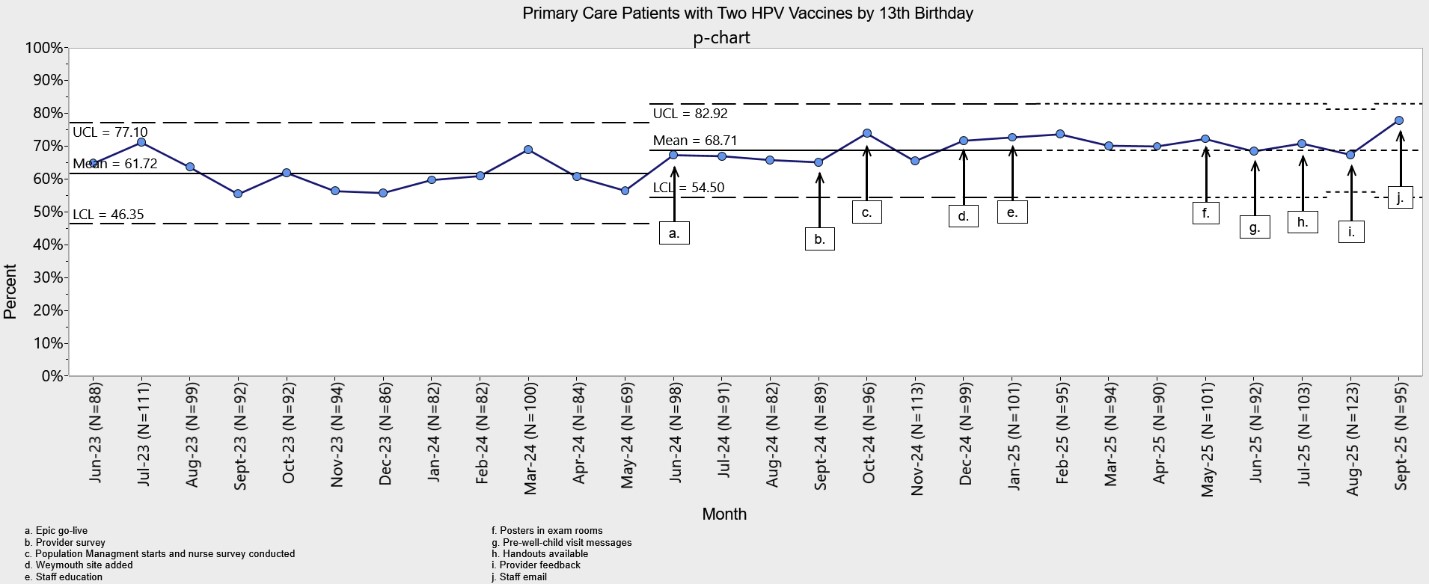
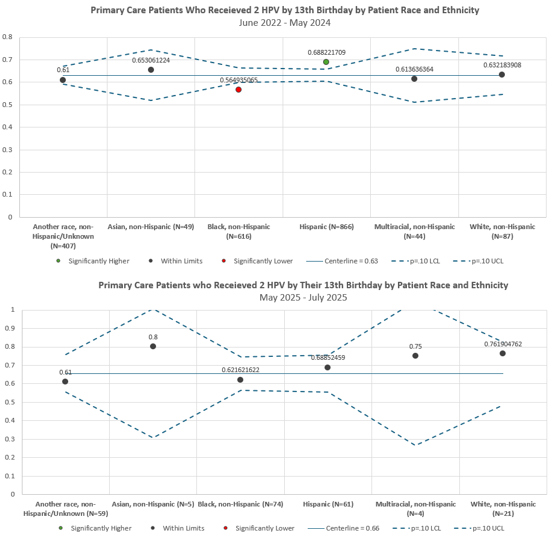
Background: Human Papillomavirus (HPV) is very common and causes multiple types of cancer. Half of those newly infected with HPV are between 15 and 24 years of age. The HPV vaccine is extremely effective, preventing more than 90% of cancers caused by HPV. However, there is growing distrust around vaccines in the US, and HPV vaccination rates tend to be lower than for other vaccines. Studies have also shown racial and ethnic disparities in both vaccine initiation and completion rates. Objective: To increase the percentage of 13 year old patients with 2 HPV vaccines from 62% to 70% by September 2025. Design/Methods: In a hospital-affiliated primary care system, we implemented a multi-disciplinary process improvement effort to improve HPV vaccine uptake between 6/1/24-9/30/25. We performed multiple PDSA cycles including educational talks, an EMR prompt, creation of a patient handout, educational video and posters, well child visit scheduling outreach and portal messages, and email feedback to providers on their performance (Figure 1). We also conducted family surveys to better understand reasons for declining the vaccine. We measured monthly completion of one and two HPV vaccines by age 13 for the population as outcome measures using statistical process control charts (p-charts). We also tracked several process measures, including administration of the vaccine at well child visits and success of scheduling outreach efforts. We tracked completion of the MCV and Tdap vaccines as a balancing measure. Finally, we conducted a pre- and post-equity analysis using cross sectional funnel plots for race and ethnicity, language, and insurance type (p=.10). Results: Completion of two HPV vaccines by age 13 increased from a baseline of 62% to 69% following implementation (Figure 2). Administration of the HPV vaccine at the 9 and 10 year visit when indicated increased from 61% to 66%. Completion of other routine adolescent vaccines remained stable at about 94%. Before the intervention a higher proportion of Hispanic patients completed the series and a lower proportion of Black patients. After the intervention this disparity was eliminated (Figure 3). In surveys (n=33) families reported concerns regarding the "newness" of the vaccine as well as a belief that it was not necessary for a child who was not yet sexually active.
Conclusion(s): A multi-pronged improvement effort increased HPV vaccine completion in a primary care setting. Future efforts should focus on effective interventions to address parental concerns.
Figure 1. Improving HPV Vaccination Rates in a Primary Care System Key Driver Diagram (KDD)
Figure 2. Percentage of patients who received two HPV vaccines by age 13
Figure 3. Pre-post comparison of HPV uptake by patient race and ethnicity

 Credit")
 photo")