Session: Technology 3: Telemedicine and Virtual Health
184 - Remote Patient Monitoring in Neonates on Nasogastric Tube Feeds: Practices, Criteria, and Barriers Across CHNC Institutions
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4181.184
Sujir P. Nayak, UTSW -Dallas, Dallas, TX, United States; Syed T. Ahmed, University of Texas Southwestern Medical School, Dallas, TX, United States; Abeer Azzuqa, UPMC Childrens Hospital of Pittsburgh, Sewickley, PA, United States; John Chuo, University of Pennsylvania Perelman School of Medicine, doylestown, PA, United States; Jeanne Zenge, University of Colorado School of Medicine, Aurora, CO, United States; Abhishek Makkar, University of Texas Southwestern Medical School, Dallas, Texas, United States, TX, United States
Assistant Professor of Pediatrics UTSW -Dallas Dallas, Texas, United States
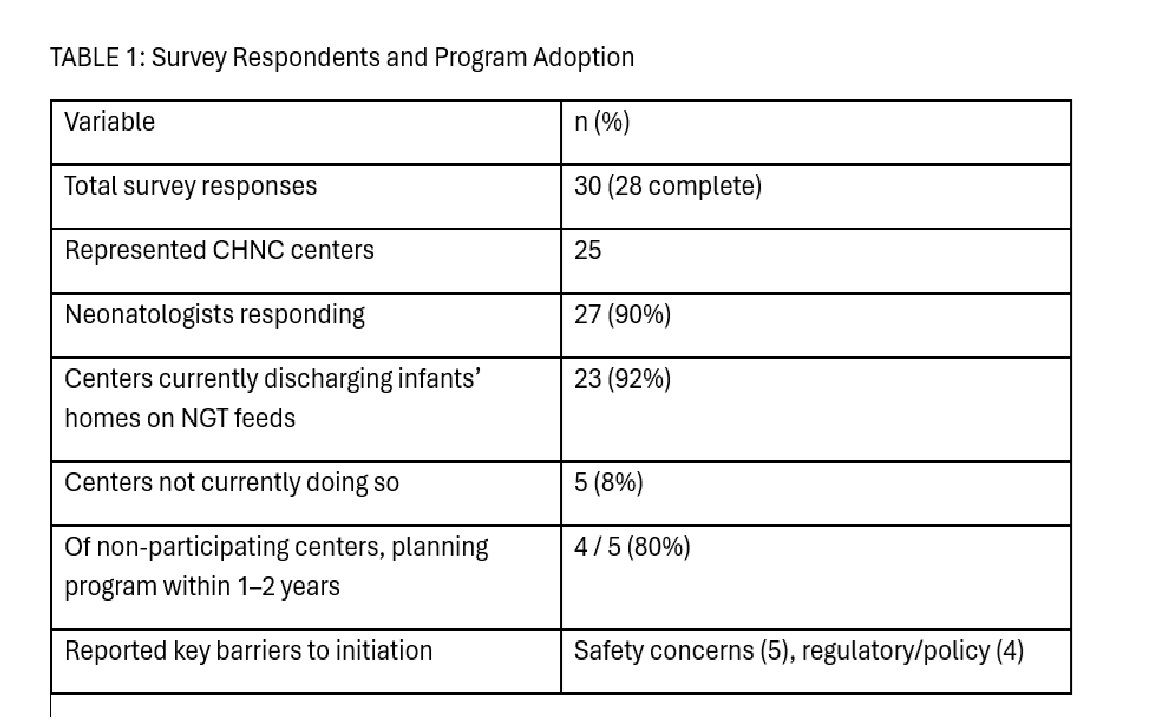
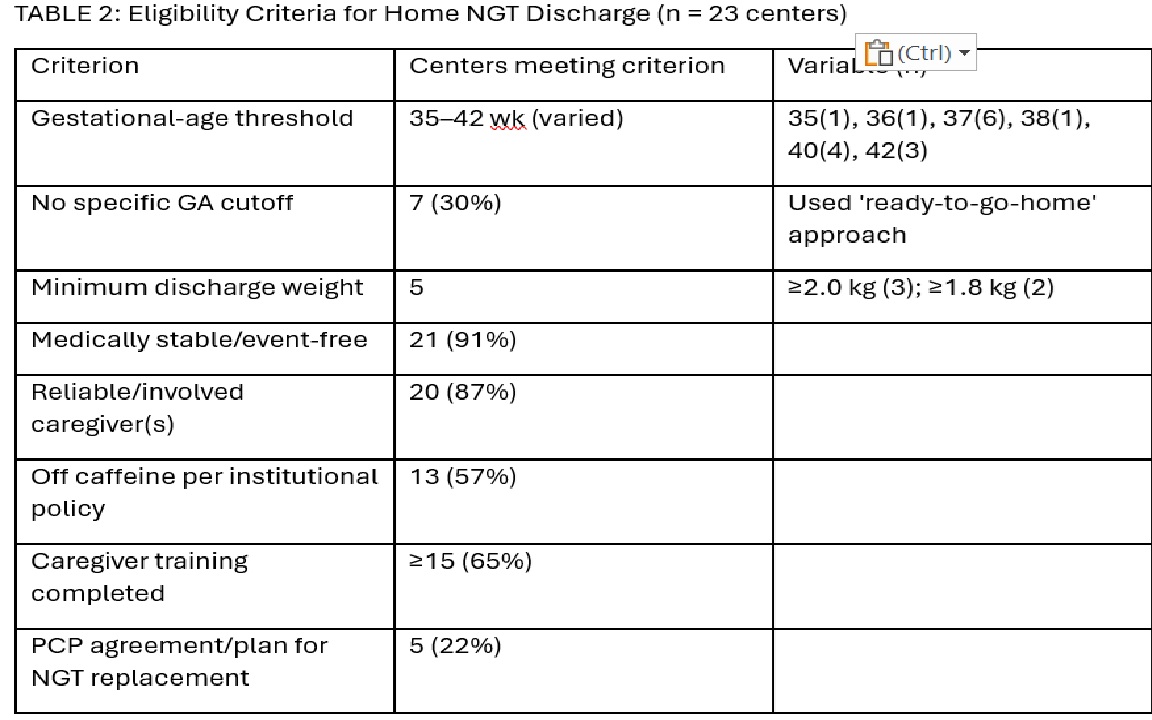
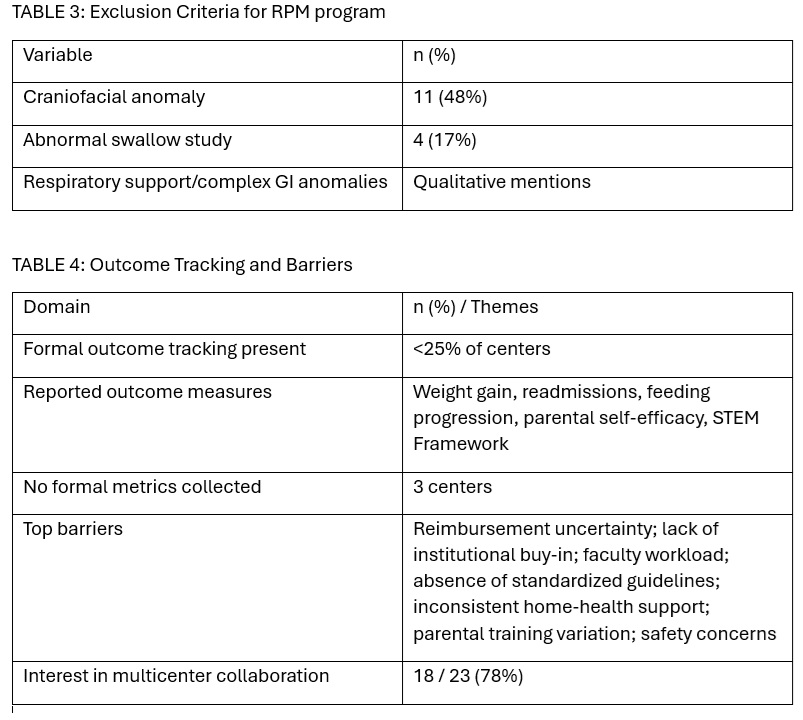
Background: Discharging neonates' home on nasogastric tube (NGT) feeds may reduce NICU length of stay and enhance family bonding, but structured remote patient monitoring (RPM) programs remain uncommon. Limited data exists on eligibility criteria, monitoring protocols, and barriers across tertiary neonatal centers. Objective: To characterize institutional practices, eligibility criteria, monitoring strategies, and perceived challenges for RPM in neonates discharged on NGT feeds across Children's Hospital Neonatal Consortium (CHNC) institutions Design/Methods: A cross-sectional, web-based survey was distributed to neonatal providers across CHNC centers. Items addressed inclusion/exclusion criteria, RPM infrastructure, follow-up frequency, outcome tracking, and barriers. Responses were collected anonymously via REDCap and analyzed using descriptive statistics Results: Thirty responses were obtained (28 complete) representing 25 CHNC center. Twenty-three (92%) centers currently discharge infants home on NGT feeds; 4 of 5 remaining plan implementation within 1-2 years. (Table 1). Eligibility criteria varied (Table 2/Table3): GA thresholds ranged from 35-42 weeks; 30% had no cutoff. Most required medical stability (91%) and reliable caregivers (87%). Minimum oral intake ranged from 0-80%; 44% allowed full tube feeds. RPM models differed by platform (Epic 6, Zoom 2, Vivify 2, LOCUS 1). Follow-up frequency ranged from weekly to monthly; monitoring duration averaged 1-3 months. Only 48% billed for RPM using codes 99214, 99453-99458. Reported barriers included reimbursement uncertainty, institutional buy-in, workload, and lack of standardized guidelines. Outcome tracking was inconsistent; < 25% captured formal metrics. Despite challenges, 78% expressed interest in multicenter collaboration. (Table 4)
Conclusion(s): RPM for home NGT-fed neonates is an emerging yet heterogeneous practice among CHNC centers. Wide variation exists in eligibility, monitoring, and sustainability. Standardized protocols and reimbursement pathways are needed to optimize safety, equity, and program scalability across neonatal systems.
Survey Respondents and Program Adoption
Eligibility Criteria for Home NGT Discharge (n = 23 centers)
Exclusion Criteria for RPM program and Outcome Tracking and Barriers