341 - Standardizing Gastrostomy Tube (GT) Teaching for Pediatric Patients and Their Caregivers
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4334.341
Gabriella Peluso, NewYork-Presbyterian Komansky Children’s Hospital, New York, NY, United States; Alim Esemenli, New York Presbyterian Weill Cornell, New York, NY, United States; Olivia Gasser, Weill Cornell Medicine, New York, NY, United States; MacKenzi Preston, Weill Cornell Medicine, New York, NY, United States; Jimin Lee, Weill Cornell Medicine, New York, NY, United States; Teresa McCann, Columbia University Vagelos College of Physicians and Surgeons, queens, NY, United States; Stephen Oh, Weill Cornell Medicine, New York, NY, United States; Snezana Nena Osorio, Weill Cornell Medicine, New York, NY, United States; Melissa Rose, Weill Cornell/New York Presbyterian, New York, NY, United States
Pediatric Resident NewYork-Presbyterian Komansky Children’s Hospital New York, New York, United States
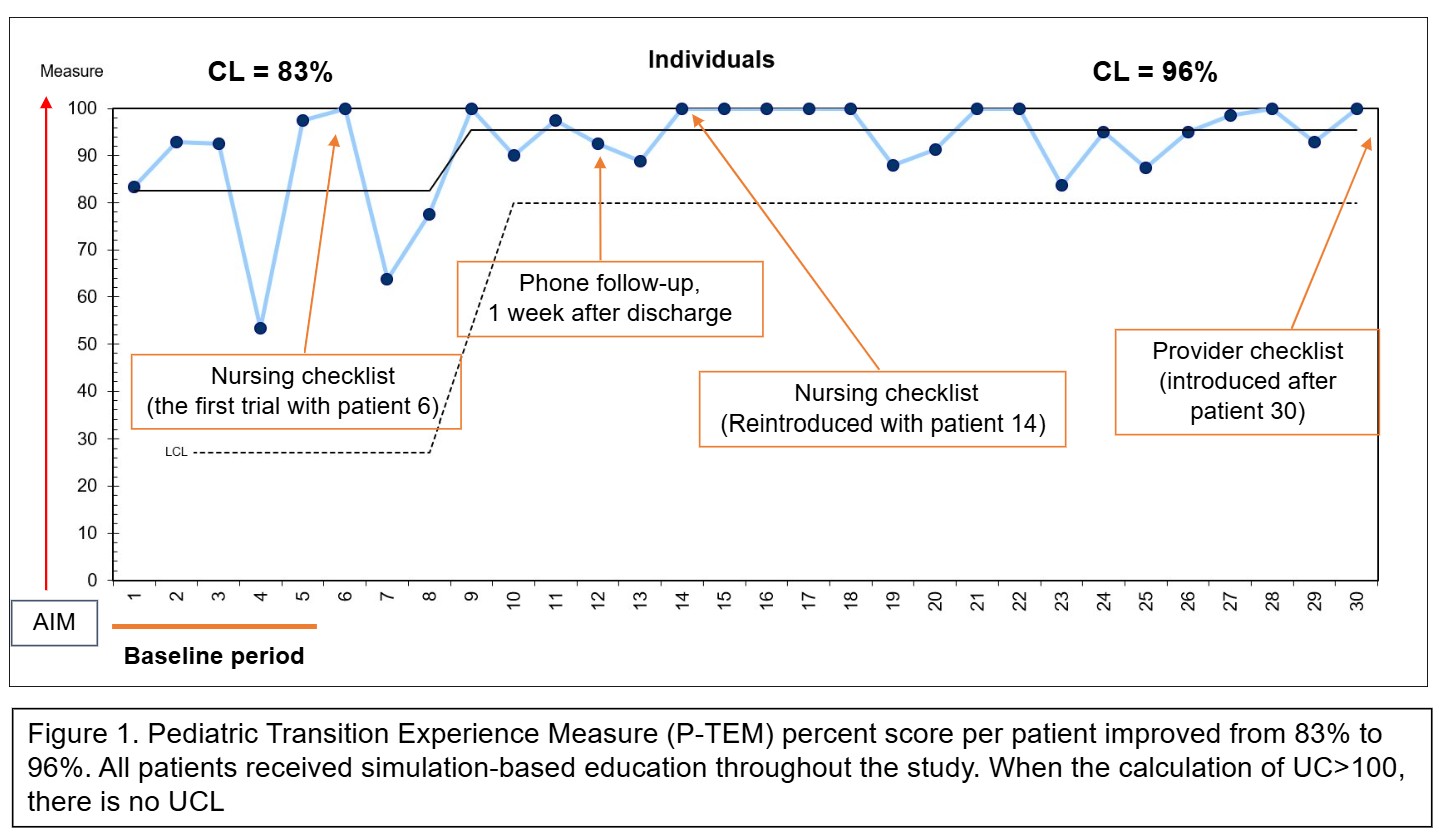
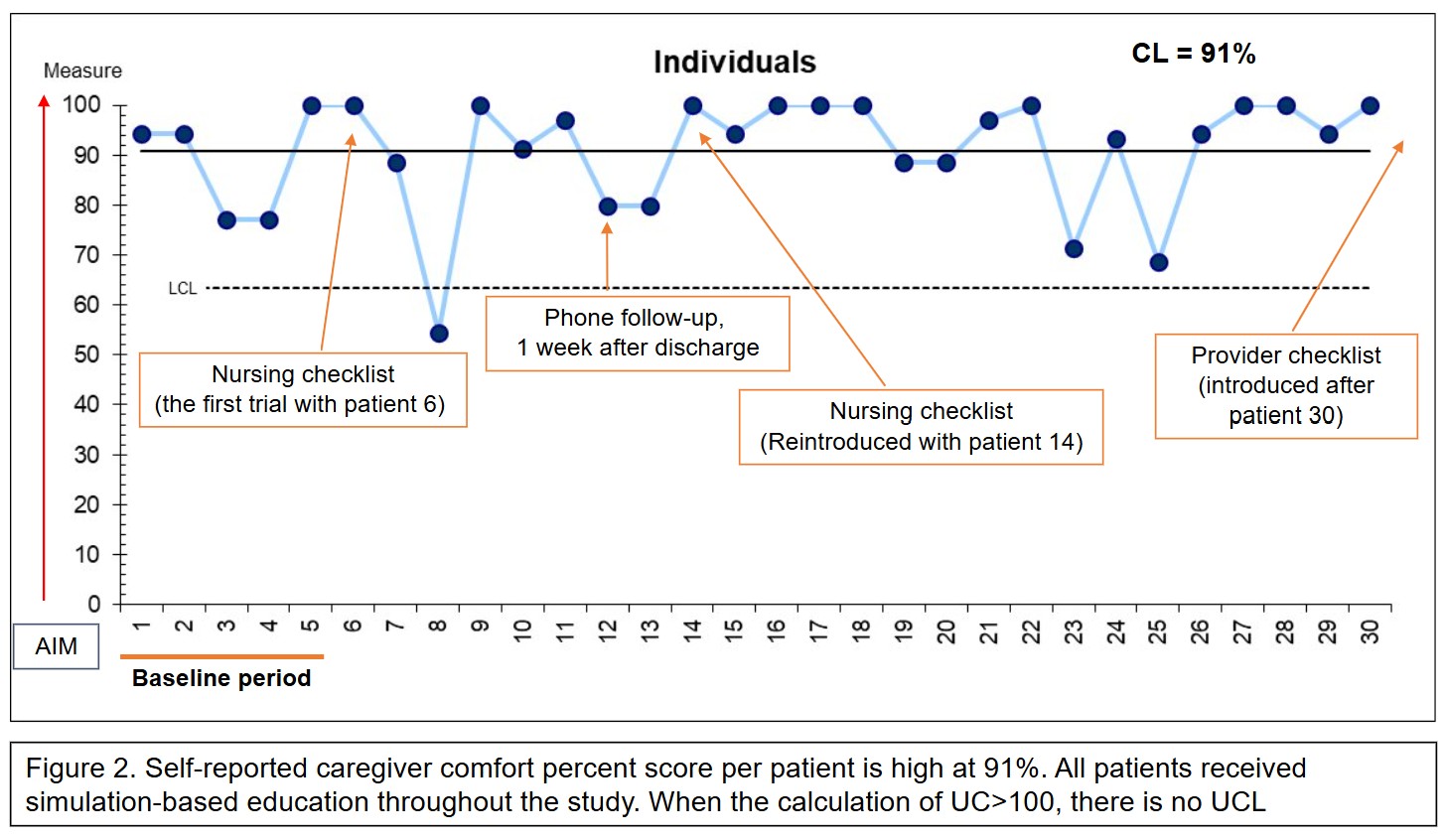
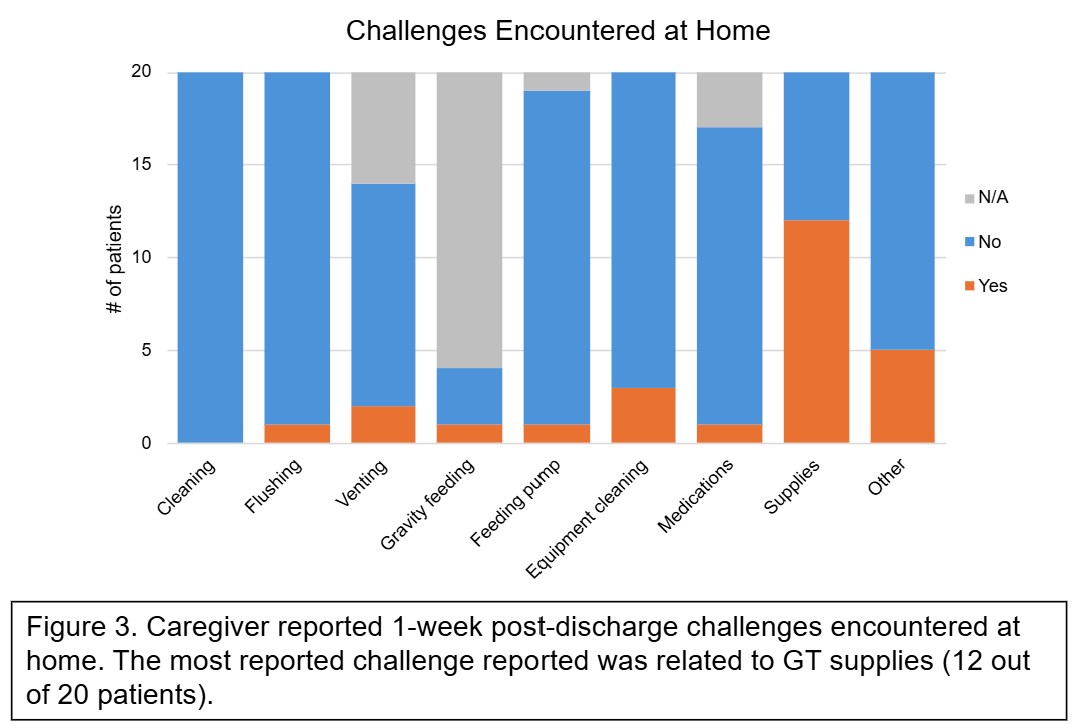
Background: Caregiver readiness is vital for safe transition from hospital to home after pediatric gastrostomy tube (GT) placement. Structured, hands-on education enhances caregiver confidence. Inconsistent discharge processes lead to variable preparedness levels, increasing the risk of complications and readmissions. Objective: To achieve the highest possible score (100%) on the Pediatric Transition Experience Measure (P-TEM), a validated caregiver-reported hospital-to-home transition quality measure, by May 2026. Design/Methods: This quality improvement project at a tertiary medical center and a community hospital used the Model for Improvement to define outcome (caregiver readiness via P-TEM and comfort with GT care), process (adherence to a 4-element GT discharge bundle), and balancing (unplanned GT-related ED visits or hospitalizations within 30 days) measures. Caregivers of patients under age 21 with newly placed GTs discharged to home were included. At baseline, all received simulation-based GT education (bundle element 1). During the intervention and via 4 PDSA cycles, three additional bundle elements were tested: 1) pre-discharge nursing assessments, 2) medical provider discharge checklist, and 3) one-week post-discharge phone calls using a survey to assess home care challenges. Demographics and P-TEM and caregiver comfort scores were collected 4-6 weeks post-discharge for all patients. EMRs were reviewed for nursing and provider documentation. Outcome and survey data were analyzed using Shewhart Individual (I) charts and descriptive statistics, with API rules applied to detect special cause variation. Results: In this study of 39 patients, patient median age was 3 years (range: 1 month to 19 years) with 56% males. Mothers were primary caregivers (90%). The majority of caregivers had no prior experience with GT care (75%). Highest level of caregiver education spans elementary school (7%), high school/GED (32%), college (36%), and graduate school (25%). We observed a special cause variation as P-TEM percentage score improved from 83% to 96% (Figure 1), while caregiver comfort score remains high and steady at 91% (Figure 2). The most reported challenge at home within 1 week of discharge was related to supply issues (Figure 3).
Conclusion(s): Sequential implementation of the GT discharge bundle improved caregiver transition readiness. Simulation-based education maintained high comfort levels, while added bundle elements enhanced readiness. Next steps: assess all four elements' impact on all study metrics including healthcare utilization and bundle adherence.

 photo")