527 - Characteristics and Medical Needs of Uninsured Pediatric Immigrant Patients Referred to Care Coordination Program Based at an Academic Tertiary Care Hospital
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4515.527
Jessica Weisz, Children's National Health System, Washington, DC, United States; Elizabeth Ireson, Children's National Health System, Washington, DC, United States; Daniel Newman, The George Washington University School of Medicine and Health Sciences, Washington, DC, United States; Hannah Miletello, George Washington University School of Medicine and Health Sciences, Arlington, VA, United States; Paola Jaminet, Children's National Hospital, Washington, DC, United States; Jennifer Robles, Children's Hospital, Washington, DC, United States; Alison Page, Children's National Health System, Washington, DC, United States; Nathalie Bernabe. Quion, Children's National Health System, Mclean, VA, United States; Sarah Durrin, Children's National Health System, Washington, DC, United States; Olanrewaju Falusi, Children's National Hospital, Washington, DC, United States; Kathy Ferrer, Children's National Hospital, Washington, DC, United States
Associate Professor Children's National Health System Washington, District of Columbia, United States
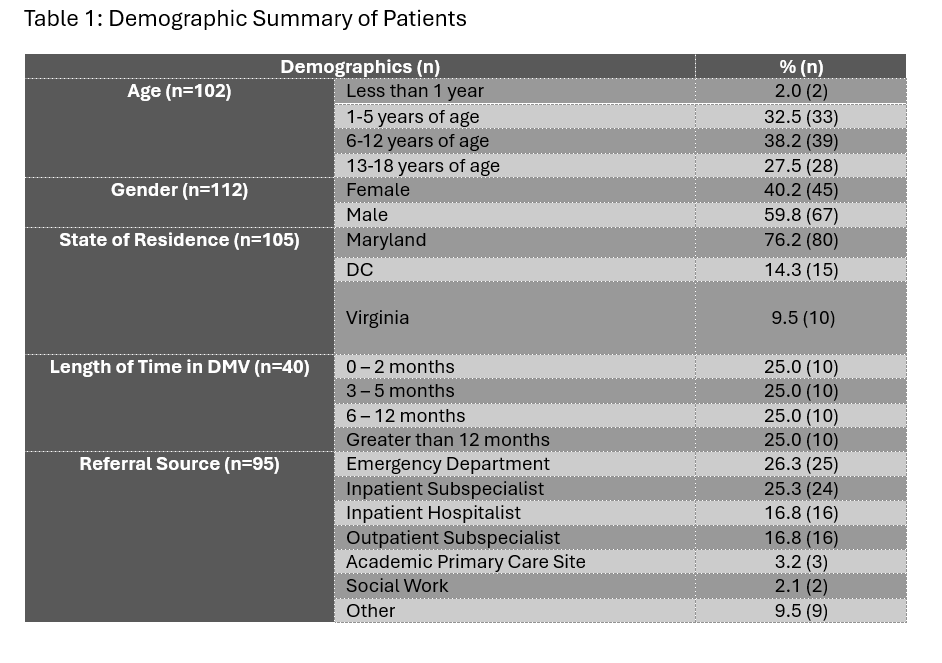
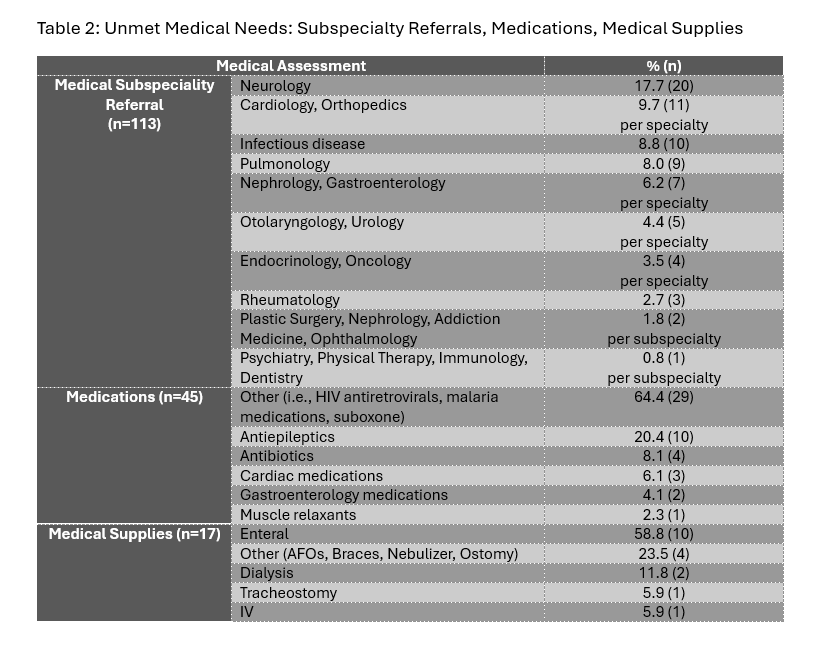
Background: Access to state-sponsored health insurance for undocumented children varies widely throughout the US (Santos, 2025). While the District of Columbia offers Medicaid-comparable insurance to income eligible children regardless of immigration status, its surrounding jurisdictions of Maryland and Virginia do not (Santos, 2025). Lack of health insurance coverage is a particular challenge; in response, Children's National Hospital created a philanthropic fund in 2019 to support access to outpatient subspecialty care, medications, and durable medical equipment for children with limited healthcare payor options due to immigration status. Objective: This study aims to describe the patients who participated in the program and how the program addresses unmet health care needs. Design/Methods: Immigrant pediatric patients with medical complexity who (1) sought health care via the emergency department (ED), hospital admission, ambulatory subspeciality care, or at mobile health unit and (2) were uninsured/self-pay were referred to the Immigrant Care Coordination team (ICC). With a newly created immigrant health coordinator role, along with social workers and physicians, the ICC team partnered with families to (1) organize medical appointments, (2) navigate the payor landscape to access subspecialty visits, prescriptions, and durable medical equipment, and (3) support families applying for financial assistance or state-sponsored insurance programs. Care coordination was tracked via REDCap, but not all data points were captured for each patient. Results: In 2024, 124 children were referred to the program; most were between ages 6-12 at the time of referral, lived in Maryland, and referred from the ED (Table 1). The most common presenting disease was seizure-activity, and the most common subspeciality referral was neurology (Table 2). Access to subspeciality appointments, medications, and medical supplies were covered as needed (Table 2).
Conclusion(s): This program serves patients with high medical complexity who lack payor coverage and have critical need for care coordination and financial assistance. Next steps are to better quantify the program's impact on health care utilization and to further evaluate how this program can adapt to evolving health care gaps.
Table 1: Demographic Information of Patients
Table 2: Unmet Medical Needs: Subspecialty Referrals, Medications, Medical Supplies

 photo")