385 - Informed Consent in Pediatric ECLS Decannulation: Variability and Implications for Withdrawal of Life-Sustaining Therapy
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4377.385
Daniel Fu, University of Chicago Division of the Biological Sciences The Pritzker School of Medicine, Chicago, IL, United States; Baddr A. Shakhsheer, University of Chicago, Chicago, IL, United States; Sean C. Wightman, Keck School of Medicine of the University of Southern California, Los Angeles, CA, United States
Medical Student University of Chicago Division of the Biological Sciences The Pritzker School of Medicine Chicago, Illinois, United States
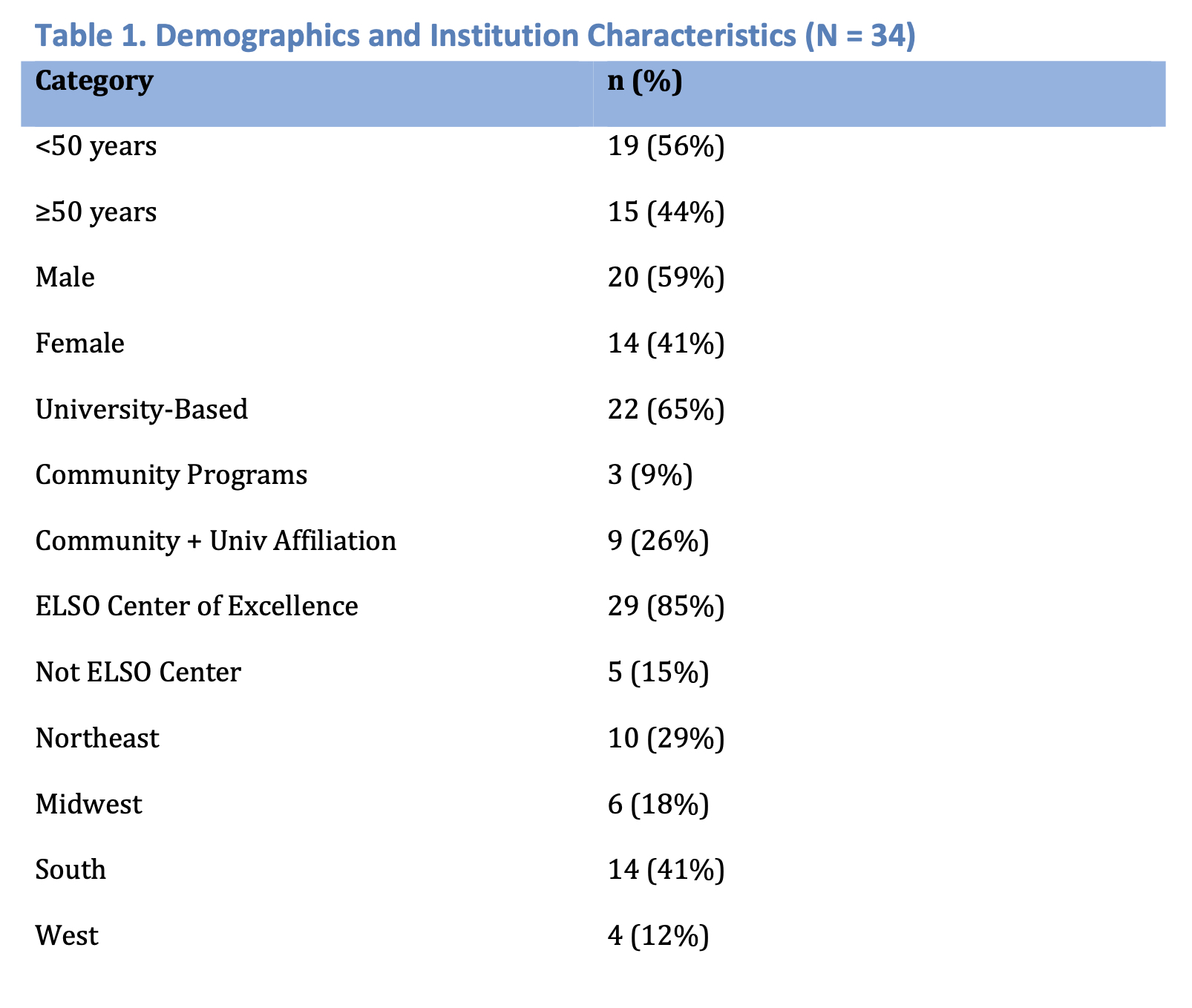
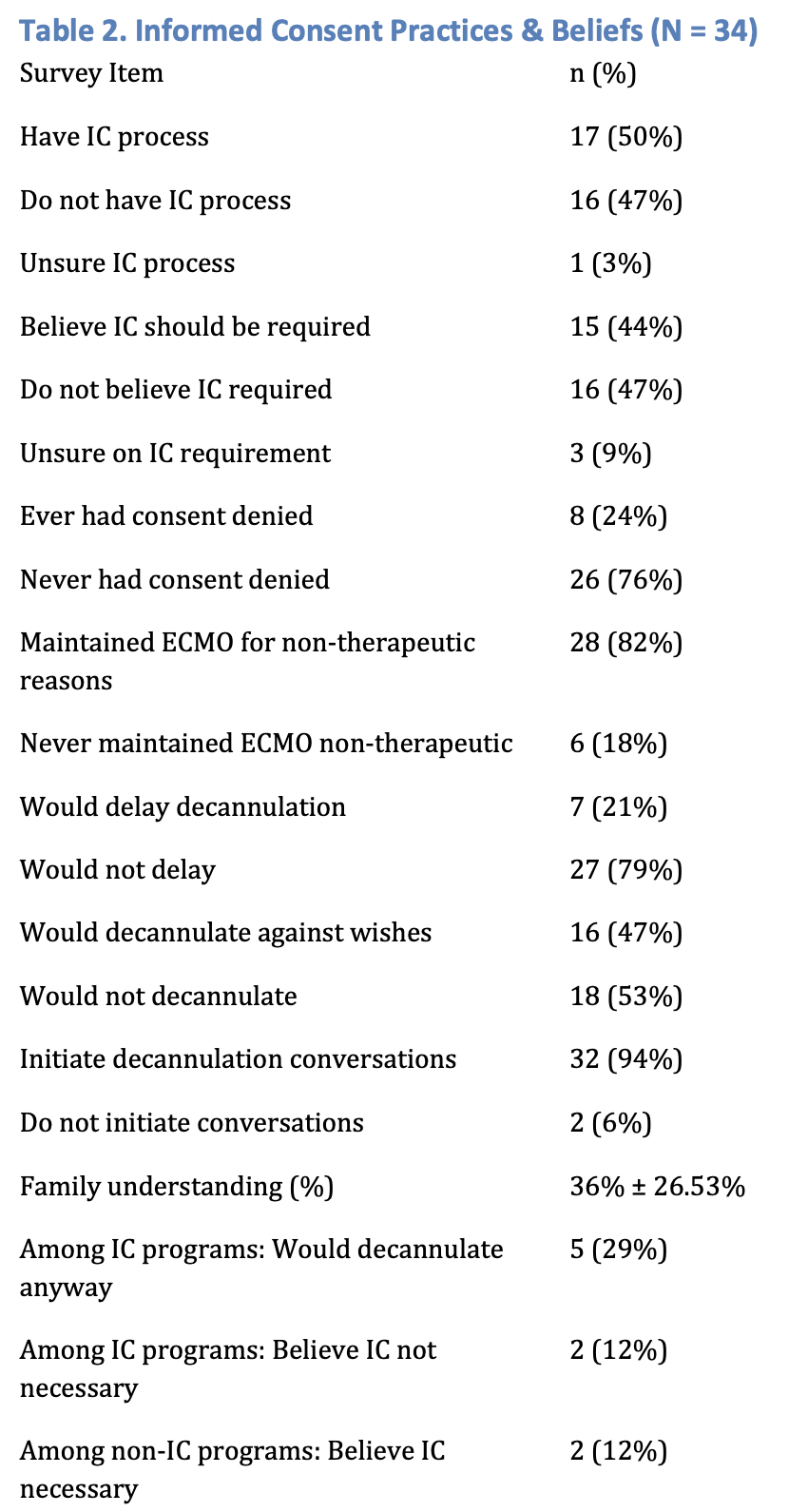
Background: Informed consent (IC) is central to medical ethics, yet its use during withdrawal of pediatric extracorporeal life support (ECLS) is inconsistent. Guidance on when IC is required, particularly in non-therapeutic scenarios, is limited. Objective: To characterize current practices, beliefs, and experiences surrounding IC during ECMO decannulation among pediatric ECMO leaders and highlight variability in clinical approaches. Design/Methods: In August 2025, a confidential electronic survey was sent to pediatric ECMO leaders. Respondents reported institutional IC practices, personal beliefs regarding consent, prior experiences with refusal of consent, and scenarios involving non-therapeutic ECMO continuation. Three clinical scenarios assessed willingness to delay or proceed with decannulation against family wishes and the frequency with which discussions about non-therapeutic decannulation were understood by families. Results: Thirty-four complete responses were analyzed. Respondents varied in age, gender, institution type, and geography; 29/34 programs were ELSO Centers of Excellence. 16 respondents reported no formal IC process, 17 reported a process, and 1 was unsure. Opinions on whether IC should be required were split (16 no, 15 yes, 3 unsure). 8 respondents had encountered refusal of consent and 28 reported maintaining ECMO for non-therapeutic reasons. In the scenario responses, 27/34 would not delay decannulation at family request, while 16/34 would decannulate against family wishes when therapy was no longer beneficial. Discussions about potential non-therapeutic decannulation were initiated by 32/34 respondents at time of cannulation but was perceived to be understood by families only 36% ± 27% of the time. Among programs with formal IC processes, 5/17 would still decannulate against family wishes, highlighting discordance between policy and practice.
Conclusion(s): Practices and beliefs regarding IC for pediatric ECMO decannulation are highly variable. Even among programs with formal consent processes, discrepancies exist between policy and clinical decision-making, especially in non-therapeutic contexts. These findings underscore the need for clearer guidance to standardize IC and preserve patient and family autonomy during ECMO withdrawal.
Figure 1: Demographics and Institution Characteristics
Figure 2: Institutional Characteristics and Beliefs

 photo")