457 - Timeline to engagement in State-Based Early Intervention services for high-risk neonatal intensive care unit graduates
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4448.457
Nicole Pouppirt, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Aneta Jedraszko, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Jessica Trenkle, Northwestern University The Feinberg School of Medicine, Chicago, IL, United States; Sarah Heigel, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Elizabeth Hoffman, Shirley Ryan AbilityLab, Chicago, IL, United States; Raye-Ann DeRegnier, Northwestern University The Feinberg School of Medicine, Chicago, IL, United States
Assistant Professor of Pediatrics Ann & Robert H. Lurie Children's Hospital of Chicago Chicago, Illinois, United States
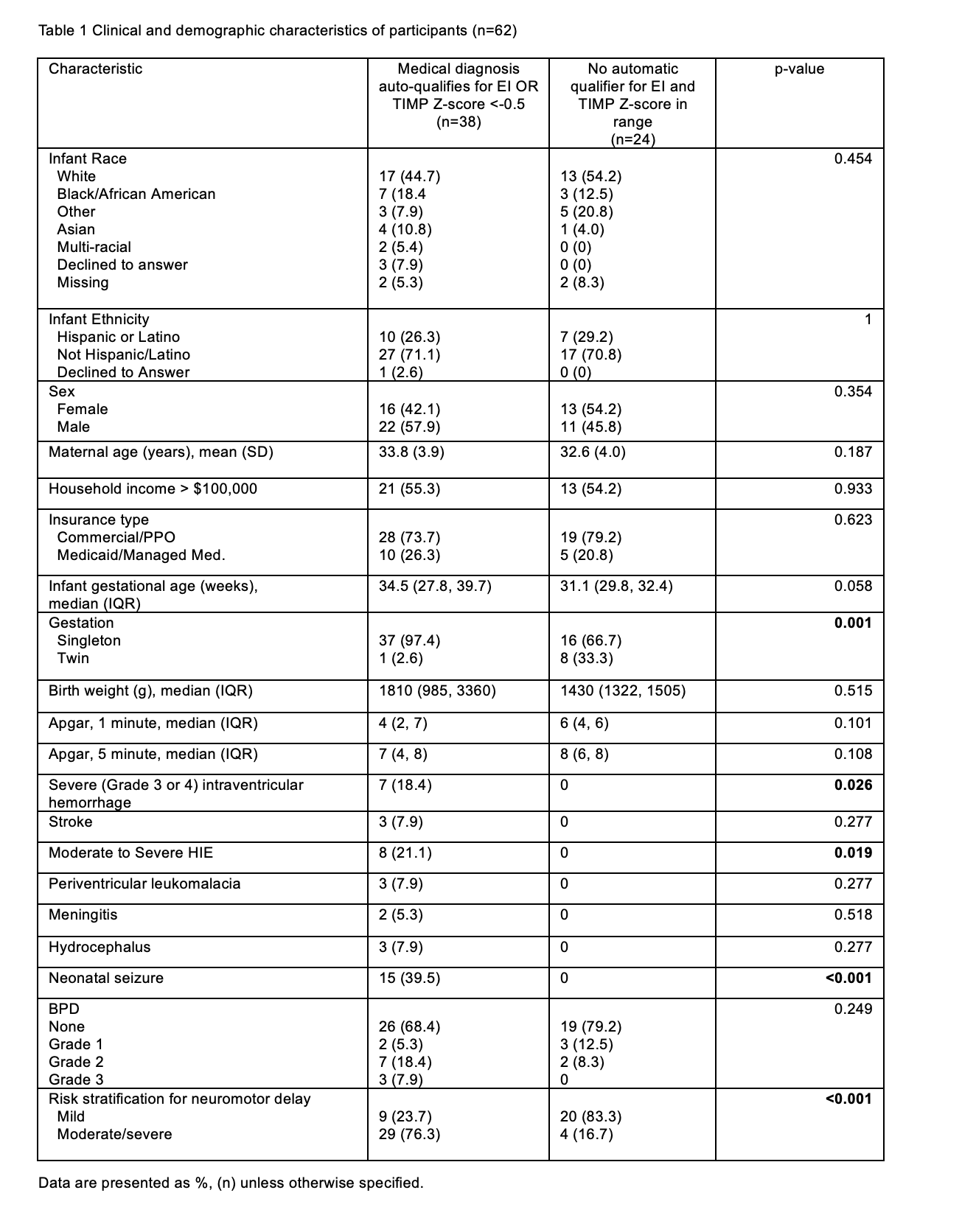
Background: Recommendations emphasize the importance of early intervention therapies beginning in infancy to enhance the brain's neuroplastic potential. Each state's Early Intervention (EI) program is federally mandated to offer therapies to families. Recognized barriers to EI participation can adversely affect infants at the greatest risk for neurodevelopmental impairment, including those discharged from neonatal intensive care units (NICU). Objective: To determine EI engagement in a cohort of high-risk NICU graduates in the first 6 months post-term age. Design/Methods: Medical and demographic data were collected from infants enrolled in a larger research study within the standard-of-care group (NCT05568264) and followed in a High-Risk Infant Follow-up (HRIF) clinic. Infants underwent the Test of Infant Motor Performance (TIMP). Descriptive statistics were used to assess EI referral and engagement. Results: The study cohort consisted of 62 participants (Table 1). More than half (35/62; 56%) had a medical diagnosis indicating high risk for developmental delay according to state definitions, automatically qualifying them for EI therapies, and 29% of infants (17/59) had a TIMP Z-score <-0.5 at 3 months CA.
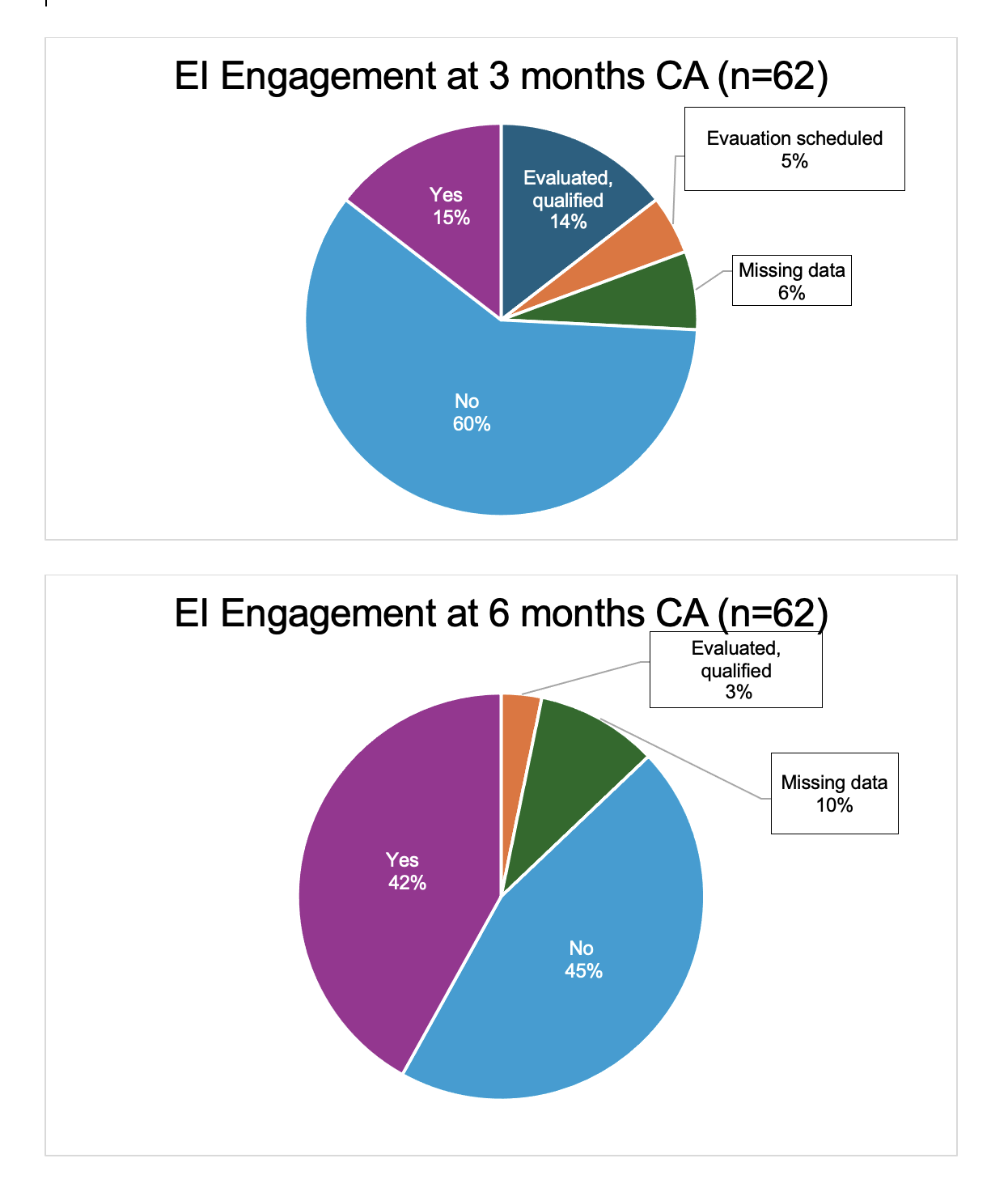
Despite these risks, only 15% of infants received EI therapies at 3 months CA (n=9/62). At 6 months CA, an improved 42% of infants had EI therapies initiated (n=26/62) (Fig. 1).
Only 24% (n=9/38) of infants with an automatically qualifying medical diagnosis or a low TIMP score were receiving EI therapies at 3 months CA, and 24% (n=9/38) either qualified or were awaiting an evaluation (Fig. 2). However, 13 infants were not receiving any therapies. Most infants not receiving EI therapies (n=9/13) received an EI referral from HRIF at 3 months CA, indicating a clinical concern. Of the 24 infants without an auto-qualifying medical diagnosis or a TIMP Z score < -0.5, only 2 were evaluated and qualified for EI at 3 months CA (Fig. 2).
Forty percent of infants with medical diagnoses at high risk of developmental delay (n=14/35) still weren't receiving EI by 3 months CA.
Conclusion(s): A small percentage of infants in the study cohort received EI therapies at 3 months CA, and therapy initiation improved by 6 months CA. Notably, a significant proportion of infants with medical diagnoses at high risk of developmental delay or with a low TIMP Z-score were still not receiving EI therapies by 3 months CA. Further studies should examine the barriers to initiating EI therapies early in infancy and determine potential solutions.
Table 1: Clinical and demographic characteristics of participants (n=62)
Figure 1: EI Engagement at 3 and 6 months Corrected Age
Figure 2: Timeline of Early Intervention (EI) engagement based on risk status *N=1 TIMP not completed

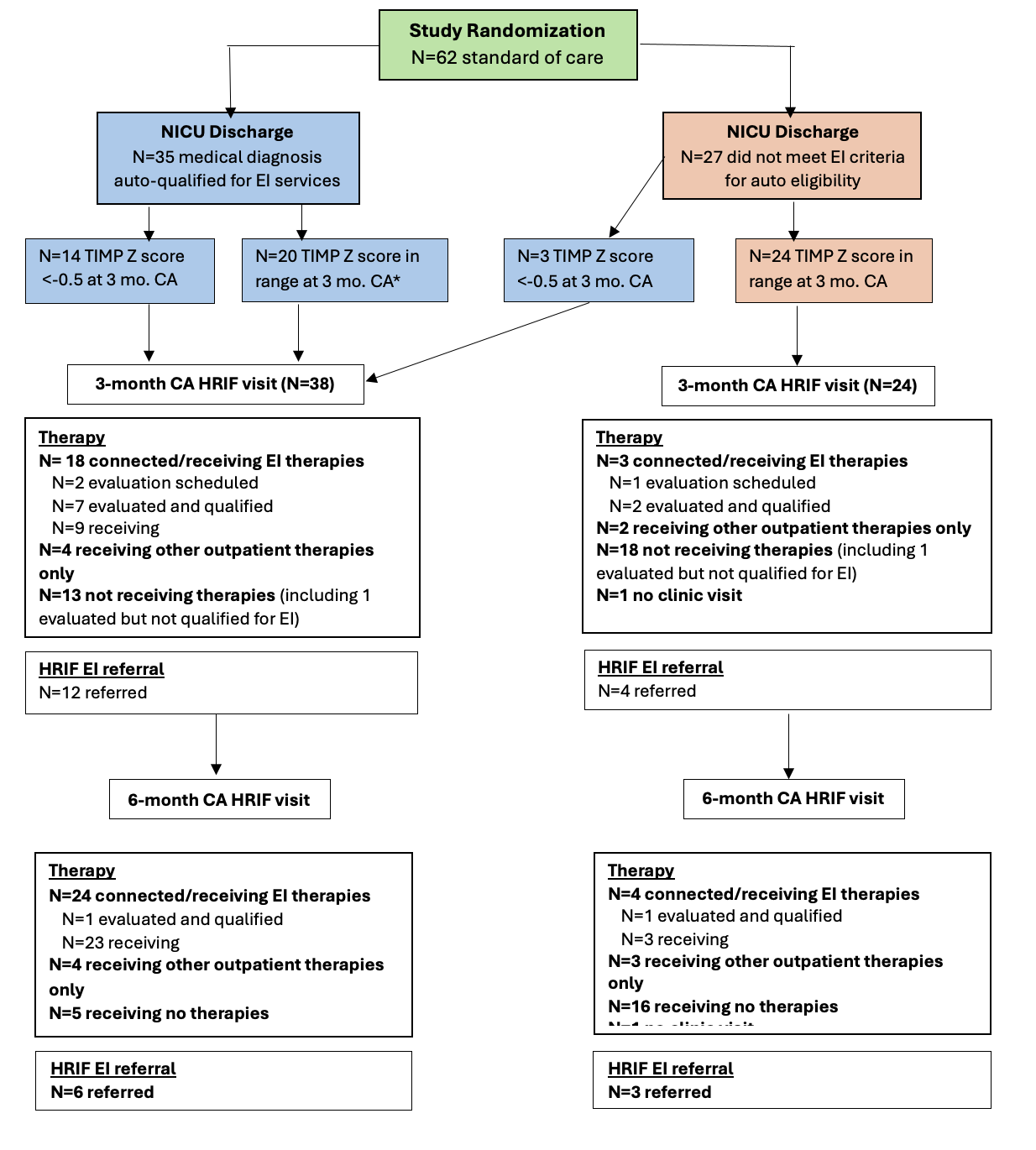 *N=1 TIMP not completed
*N=1 TIMP not completed 