108 - Improving Admission Normothermia for Infants <32 Weeks at a Community Level III NICU
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4106.108
Sneha Taylor, CHOC Children's Hospital of Orange County, Orange, CA, United States; Jennifer M. Potts, Riverside Community Hospital - - Riverside, CA, Riverside, CA, United States; Amanda Doyle, Riverside Community Hospital, Oak Hills, CA, United States; Jeycee Basilio, Riverside Community Hospital, Riverside, CA, United States
Attending Neonatologist CHOC Children's Hospital of Orange County Orange, California, United States
Background: Both hypothermia and hyperthermia increase morbidity and mortality among preterm infants. Our unit's admission normothermia rate for infants < 32 weeks or ≤1500 g was 55%, below the CPQCC benchmark of 75%.
Local Problem: Inconsistent temperature management practices-unprepared transport incubators, cold rooms, inconsistent use of thermal aids-, limited pre-admission readiness, and variable staff awareness contributed to temperature instability. Setting: Level III community NICU, 35 beds, Avg CPQCC babies ~60 per year Objective: SMART
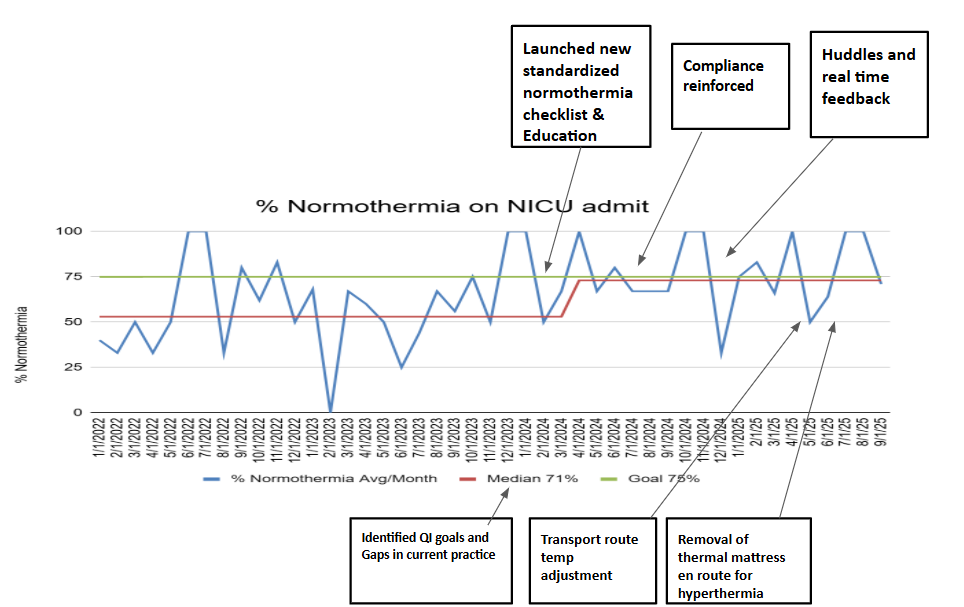
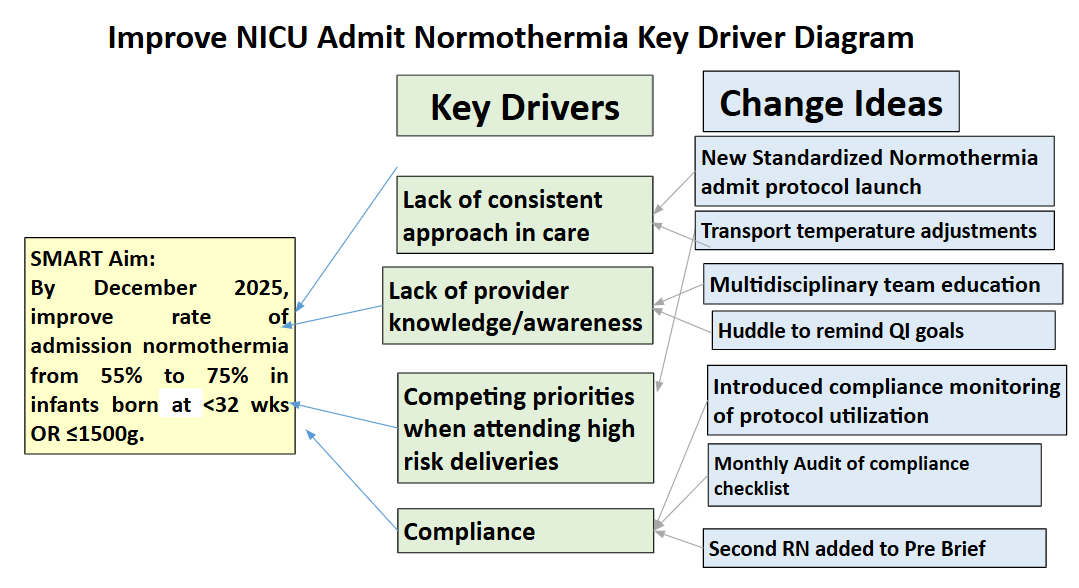
Aim: To improve admission normothermia from 55% to 75% by December 2025 through evidence-based, multidisciplinary interventions. Design/Methods: All inborn infants < 32 weeks or ≤1500 g were included, with an average of N=5 per month. Using the DMAIC framework, the team analyzed workflow gaps and temperature data. Interventions were implemented through 5 PDSA cycles: Cycle 1 (Feb-Mar 2024): Introduced multidisciplinary education and a pre-admit checklist. Cycle 2 (May 2024): Encouraged checklist compliance. Cycle 3 (Sept 2024): Discussed normothermia goals during huddles and started giving immediate feedback. Cycle 4 (March 2025): Transport route temperature adjustments added. Cycle 5 (June 2025): Removal of thermomattress during transport for hyperthermia initiated. Process and outcome measures consisted of admission normothermia, checklist compliance, and the occurrence of hyperthermia. Results: Admission normothermia improved from 55% (2023) to 71%(goal 75%) (Sept 2025). Checklist compliance reached 88%(goal 90%), and hyperthermia rose to 15%(goal 10%). The audit showed that the most temperature swings occurred during long trips from the delivery room to the NICU, mostly because staff sometimes forgot to check probe placement or adjust the incubator settings as needed. Overheating in infants over 28 weeks was noted when both a thermomattress and plastic wrap were used. High census and staff shortages are also noted to be contributing factors in recent months.
Conclusion(s):
Discussion: Structured education, standardized checklist, and accountability improved temperature management, but sustaining compliance remains challenging. This project highlighted that behavior-based reinforcement and system checks are essential for reliable temperature stability.
Conclusion: Normothermia rates at admission in a community NICU were improved by a multidisciplinary team, standardized protocol, and data-driven approach. Continuous monitoring and reinforcement are required to maintain the gains and reduce temperature extremes.

 Credit")
 photo")