70 - Screening and Addressing Food Insecurity: A Quality Improvement Project at an Academic Pediatric Primary Care Clinic
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4068.70
Mia C. Feller, MedStar Georgetown University Hospital, Washington, DC, United States; Janine A. Rethy, Georgetown University School of Medicine, Washington, DC, United States; Sejal Bavishi, Medstar Georgetown University Hospital, Washington, DC, United States; Danielle R. Abraham, Georgetown University School of Medicine, Arlington, VA, United States; Joanne S. Odom, Georgetown University School of Medicine, Washington, DC, United States; Janet Osherow, DC Metro Therapists, LLC, Silver Spring, MD, United States; Nichelle Johnson, MedStar Georgetown University Hospital - Kids Mobile Medical Clinic, Washington, DC, United States; Shelby Wyand, Medstar Health Research Institute, Columbia, MD, United States; Ahmed A. Deyab, MedStar Health, Laurel, MD, United States; Stephen Fernandez, MedStar Health Research Institute, Columbia, MD, United States; Ami Patel, Georgetown University School of Medicine, Washington, DC, United States
Pediatrics Resident MedStar Georgetown University Hospital Washington, District of Columbia, United States
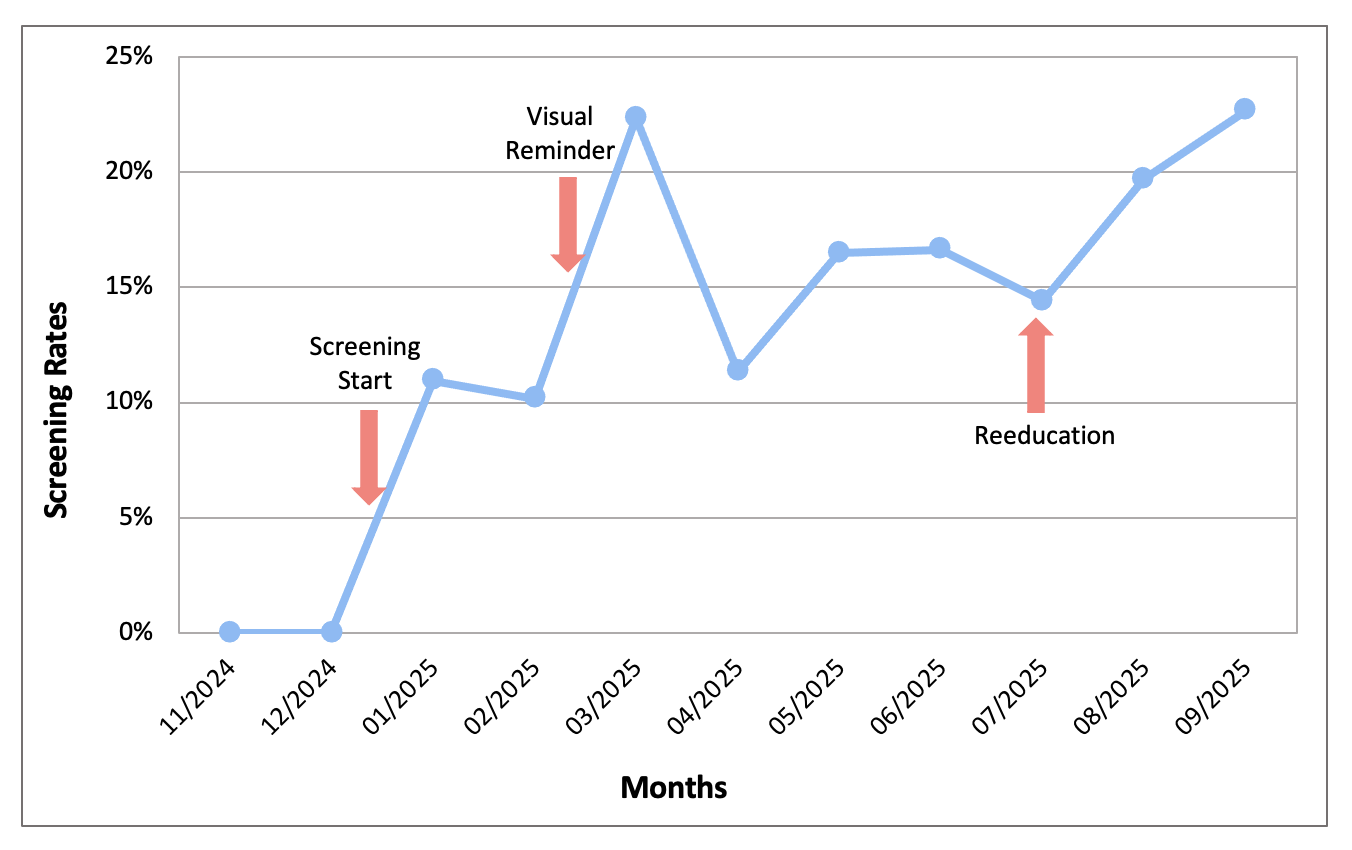
Background: Food insecurity (FI) is associated with poor health outcomes, affecting 1 in 7 children in the USA. The American Academy of Pediatrics recommends universal screening for FI using Hunger Vital Sign™ (HVS) - a validated 2-question screen, but implementation in academic clinical settings is challenging. In the pilot phase of this study, a needs assessment was conducted on 78 representative families with 17% positive for FI (FI+), preferences for electronic (72%) vs. verbal screening (53%) and for grocery gift cards (92%) and farmers markets (77%). Objective: To implement universal FI screening at an urban academic pediatric primary care clinic, increase screening rates with quality improvement interventions, and create sustainable structures to address FI with connection to local resources and a health system produce prescription program (PRx). Design/Methods: In this IRB-approved study, universal FI screening during well checks was initiated on 1/2025. Prior to initiation, the EMR was optimized to include HVS and referrals to social worker (SW) and PRx, a clinic-specific workflow and resource list was developed, and in-house provider training was completed. Caregivers are verbally screened with HVS during visits and provided resources and referrals to SW if FI+. SW ensures optimal utilization of resources and determines eligibility for PRx, including gift cards to farmers markets and produce delivery. To increase screening rates, 2 PDSA cycles were conducted with visual reminders in 3/2025 and formal provider reeducation in 7/2025. Screening data was reviewed through 9/2025. Results: 868 patients were screened, with 6% FI+. The 1st PDSA cycle of visual reminders increased screening rates from 10% to 22%. The 2nd PDSA cycle of reeducation increased screening rates from 14% to 20%, with a sustained increase to 23% following (Figure 1). 38 SW referrals were made, with 10 families enrolled into PRx.
Conclusion(s): This study highlights that implementation of a new screening tool in a busy and diverse academic clinic is a multi-faceted process requiring significant tailoring to address barriers to successful universal screening. While screening rates were lower than desired, significant barriers - time constraints, lack of provider engagement, and inability to integrate into patients' pre-arrival intake process - were identified throughout implementation. Addressing identified barriers through PDSA cycles improved screening rates. This study successfully connected FI+ patients with resources, SW support, and PRx with potential to identify and support additional families as screening rates continue to increase.

 Credit")