391 - Measuring family-centered care practices across 99 NICUs: Are resources and acuity correlated with family empowerment?
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4383.391
Malathi Balasundaram, Stanford University School of Medicine, Mountain View, CA, United States; Morgan E. Kowalski, Stanford Medical Center, Clemson, SC, United States; Laura Hedli, Stanford University School of Medicine, Palo Alto, CA, United States; Annie Janvier, Université de Montréal, CHU Sainte-Justine, Montréal, PQ, Canada; Keira Sorrells, NICU Parent Network, Lanesville, IN, United States; Mia Malcolm, Ollie Hinkle Heart Foundation, St. Louis, MO, United States; Jessica Liu, Stanford University School of Medicine, Palo Alto, CA, United States; Henry Lee, University of California San Diego, La Jolla, CA, United States
Clinical Professor Stanford University School of Medicine Mountain View, California, United States
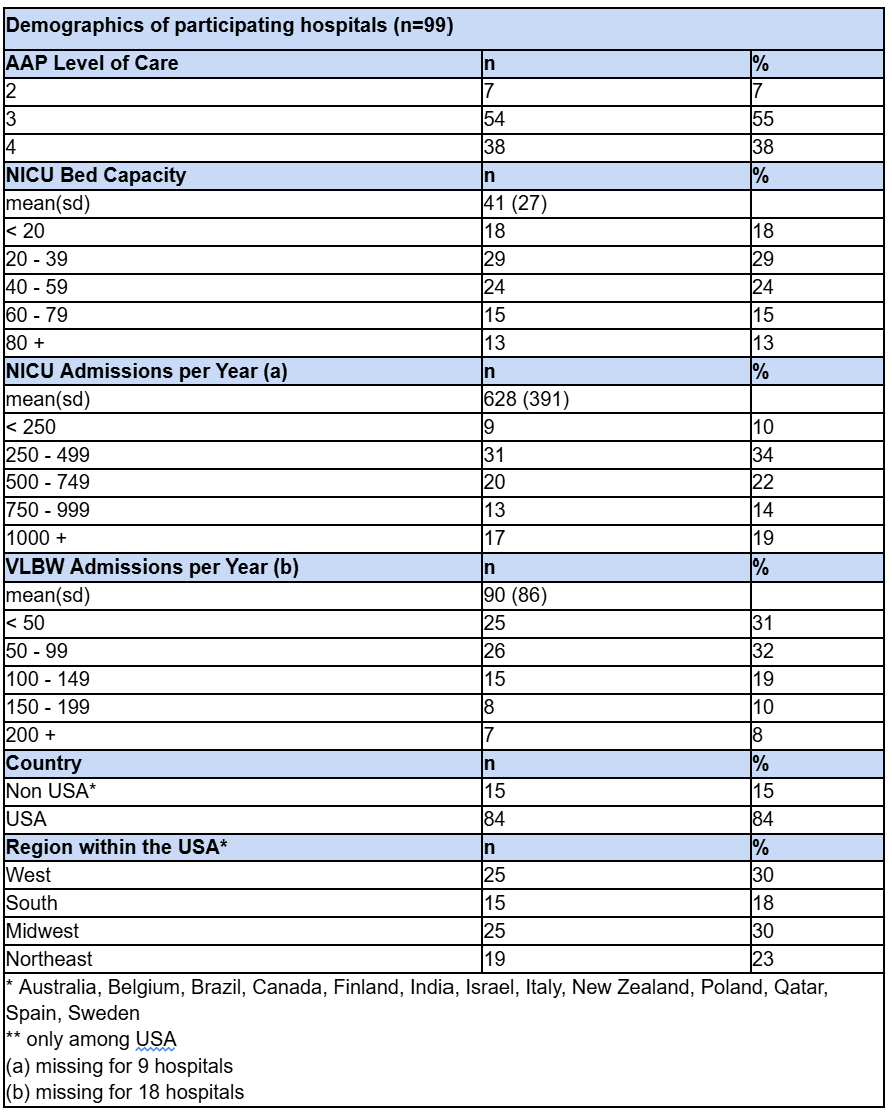
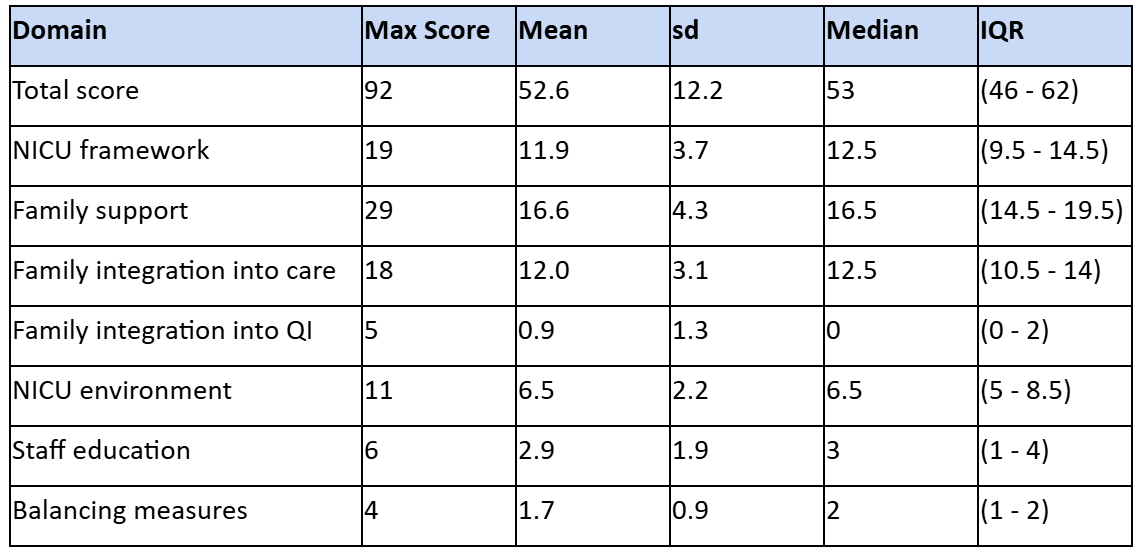
Background: Family-Centered Care (FCC) in the Neonatal Intensive Care Unit (NICU) promotes parental participation in infant care. Evidence shows FCC to have improved infant growth, reduced stress and infection rates, shorter stays, and fewer readmissions. Despite these benefits, there is no standardized approach to measure or benchmark FCC practices across NICUs. Objective: To explore the current state of FCC delivery and identify pilot benchmark practices across NICUs. Design/Methods: This cross-sectional, descriptive study was conducted by the international FCC Taskforce, an international, multicenter, collaborative solely focused on FCC in the NICU, and approved by the Stanford IRB. Multidisciplinary clinicians and NICU families co-developed a REDCap survey encompassing seven FCC domains: (1) framework/infrastructure, (2) family support, (3) family integration into care, (4) family integration into quality improvement (QI), (5) NICU environment, (6) staff education, and (7) process measures. The survey was distributed globally in October 2024 to NICU clinical leaders. Each domain was scored based on responses. Differences across hospital factors were assessed using t-tests, ANOVA, Wilcoxon rank-sum, and Kruskal-Wallis tests (SAS v9.4). Results: A total of 99 NICUs participated (84 U.S.-based, 15 international). Table 1 shows the demographics of participating NICUs. Significant variation in FCC practices was observed across all domains. (Table 2) The framework/infrastructure domain showed the highest scores, indicating that many NICUs have organizational structures supporting FCC (e.g., FCC Committees, Family Advisory Councils, access to social workers and mental health professionals). The lowest scores were found in family integration into QI, where many NICUs reported having no processes in place.Higher NICU capacity (beds and admissions) was positively correlated with higher FCC domain scores across all areas except staff education.(not shown) Similarly in Figure 1, NICUs with a higher American Academy of Pediatrics (AAP) level of care scored significantly higher in framework/infrastructure, family support, and family integration into QI, but not in family integration into care, staff education or process measures.
Conclusion(s): Wide variation exists among NICUs in the delivery of FCC. While higher-level NICUs demonstrate stronger infrastructure and more clinician presence, these advantages do not necessarily correlate to greater family integration into care or enhanced staff education regarding FCC. Strengthening these domains may be key to achieving true family-centered excellence.
Demographics of participating hospitals
Distribution of Domains' scores
Figure 1: Domain scores differences based on AAP Level of Care

 photo")
.jpg)
