475 - Early Blood Carbon Dioxide Levels and Later Neurological Diagnoses in Infants With Perinatal Asphyxia
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4466.475
Eliisa Löyttyniemi, University of Turku, Turku, Varsinais-Suomi, Finland; Vilhelmiina Parikka, University of Turku, Turku, Varsinais-Suomi, Finland; Niina Viitaharju, university of turku, Turku, Varsinais-Suomi, Finland; Bishwesvar Singh, University of Turku, Turku, Varsinais-Suomi, Finland; Kjell Helenius, University of Turku and Turku University Hospital, Turku, Varsinais-Suomi, Finland
Biostatistician University of Turku Turku, Varsinais-Suomi, Finland
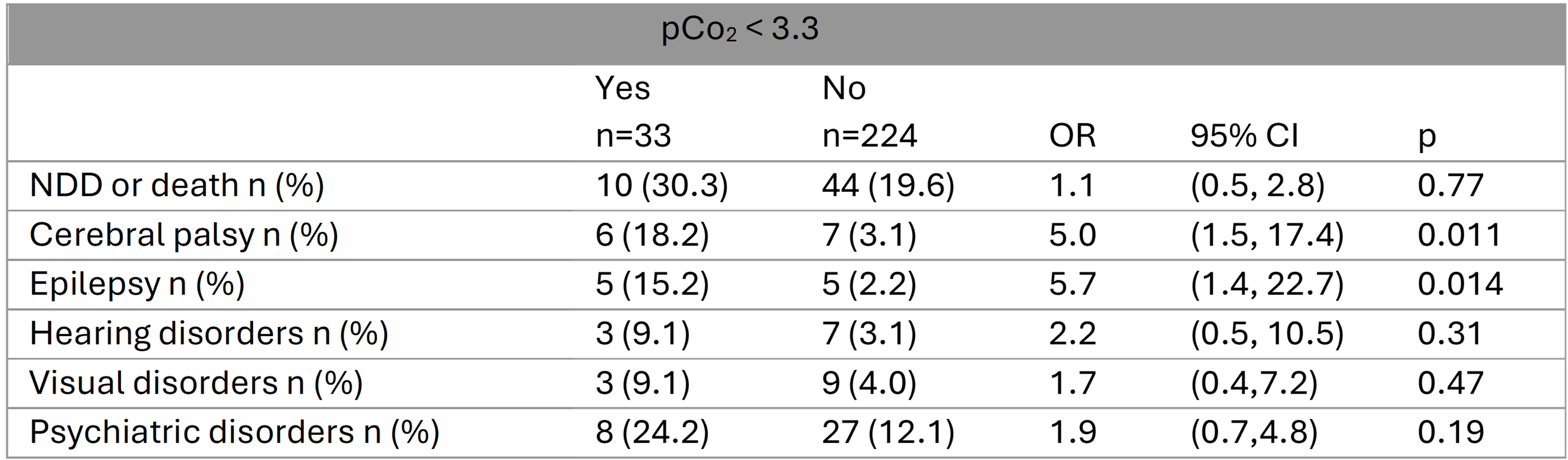
Background: Perinatal asphyxia (PA) can lead to hypoxic-ischemic encephalopathy (HIE), with the most serious outcomes being neonatal death or severe disability. Low pCO2 (hypocarbia) causes cerebral vasoconstriction and has been linked to brain injury and adverse outcomes in infants. Objective: The aim of this study was to investigate the possible association between occurrence of low blood pCO2 levels ( < 3.3 kPa ≈ 25 mmHg), measured during the first 72 hours after birth in infants with PA (with or without HIE), and subsequent neurological diagnoses. Design/Methods: The study included 257 infants born at ≥36 gestational weeks in a single-center, university level hospital in Finland between January 2010 and June 2022. All infants had a diagnosis of perinatal asphyxia (ICD-10 category P21), with a median follow-up time of 10.8 years. pCO2 values during the first 72 hours after birth and subsequent neurological diagnoses were obtained from hospital records as follows: cerebral palsy (ICD-10 codes G80-83), epileptic disorders (G40-41), psychiatric disorders (F70-98), visual disorders (H47-49, H53-55), and hearing disorders (H90-91). In addition to individual diagnoses, a composite outcome of all neurodevelopmental disorders (NDD) or death was analyzed using logistic regression, adjusted for therapeutic hypothermia, sex, and mode of delivery. Odds ratios (ORs) were estimated with 95% confidence intervals (CIs). Results: Of these 257 infants, 148 (58%) were male, with a median birth weight of 3585 grams. The median 5-minute Apgar score was 5. Forty-four infants received therapeutic hypothermia, of whom five died. Fifty-four infants (21%) had NDD, 13 (5%) cerebral palsy, 10 (4%) epilepsy, 10 (4%) hearing disorders, 12 (5%) visual disorders, and 35 (14%) psychiatric disorders. Thirty-three infants (13%) had at least one pCO2 value below 3.3 kPa. Among these, 6 (18%) had cerebral palsy and 5 (15%) had epilepsy, compared with 3% and 2%, respectively, among infants with lowest pCO2 ≥ 3.3 kPa. After adjustment, low pCO2 levels ( < 3.3 kPa), were significantly associated with cerebral palsy (OR 5.0, 95% CI 1.5 - 17.4) and epilepsy (OR 5.7, 95% CI 1.4 - 22.7). Low pCO2 levels were not significantly associated with hearing, visual, psychiatric disorders or composite outcome.
Conclusion(s): Early pCO2 levels may serve as a predictor of long-term neurological outcomes, such as epilepsy and cerebral palsy, in infants with perinatal asphyxia.
Table 1. Occurrence of neurodevelopmental diagnoses in infants with perinatal asphyxia (n=257) using a pCO2 threshold of 3.3 kPa (≈ 25 mmHg). Odds ratios (ORs) with 95% confidence intervals were estimated using logistic regression, adjusted for therapeutic hypothermia, sex, and mode of delivery.
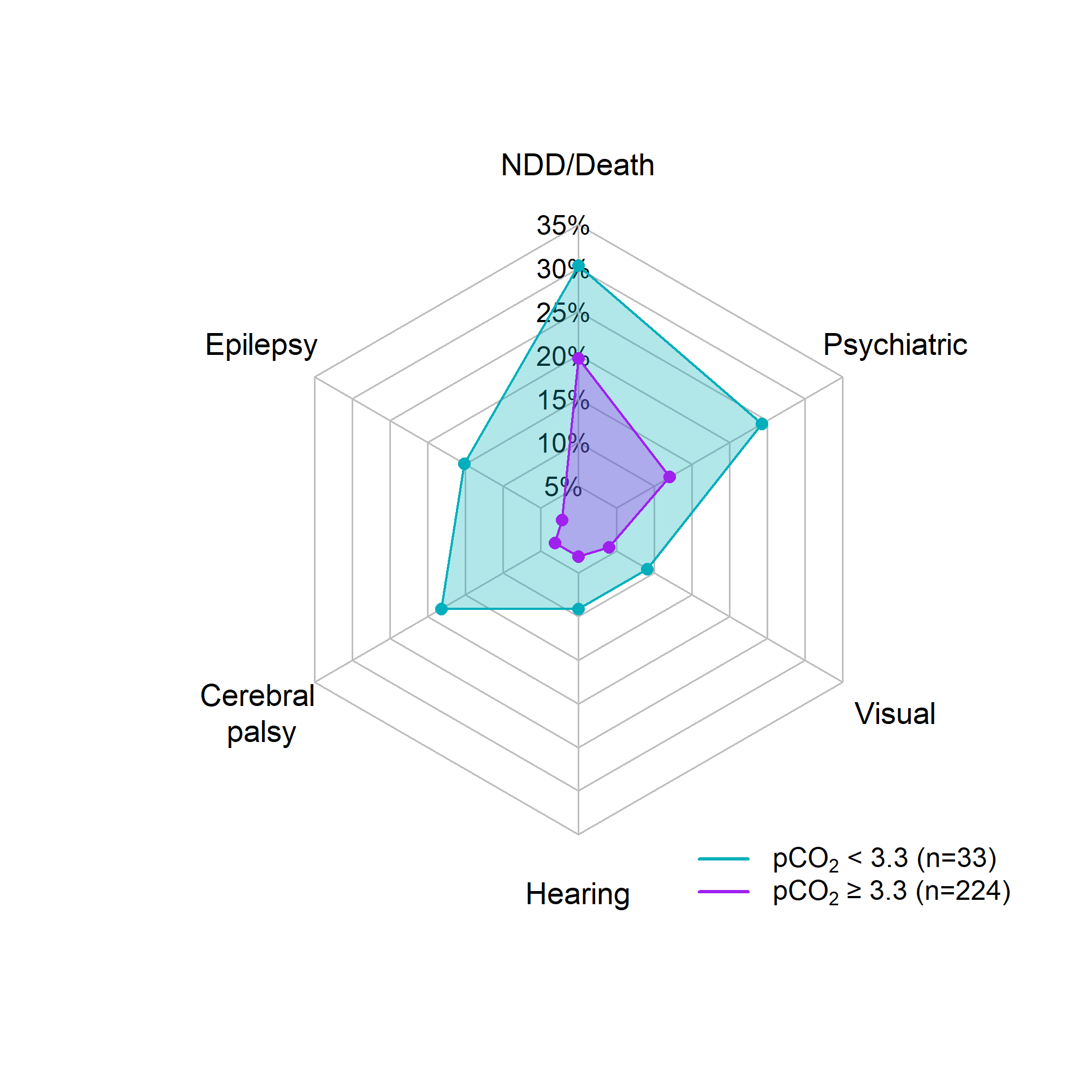
Figure 1. Occurrence of neurodevelopmental diagnoses (NDD) in infants with at least one pCO2 measurement below 3.3 kPa (≈ 25 mmHg) and those infants whose all pCO2 values were at least 3.3 kPa. All infants had a diagnosis of perinatal asphyxia, with or without HIE (n=257).

 photo")