577 - Food Insecurity and Pharmacotherapy Among Youth with Obesity
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4565.577
Parisa Afsharian, Harvard Medical School, Cambridge, MA, United States; Lauren Fiechtner, MassGeneral Hospital for Children, Boston, MA, United States; Cornelia Griggs, MassGeneral Hospital for Children, Boston, MA, United States; Allison Wu, Boston Children's Hospital, Boston, MA, United States; Rachel Whooten, MassGeneral Hospital for Children, Boston, MA, United States
Medical Student Harvard Medical School Cambridge, Massachusetts, United States
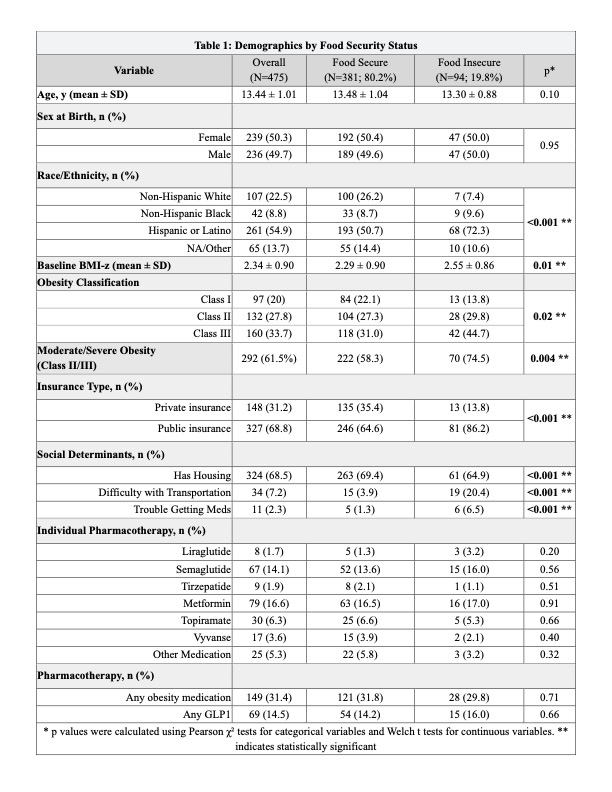
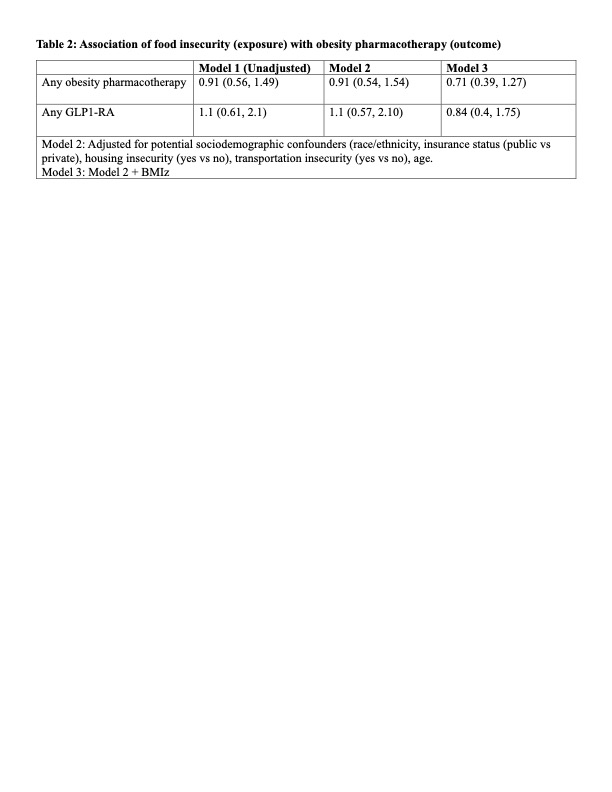
Background: Food insecurity is linked to barriers in healthcare access and obesity treatment among adults, but its relationship to obesity pharmacotherapy in youth is poorly understood. Pediatric obesity pharmacotherapy, including glucagon-like peptide-1 (GLP-1) receptor agonists, is rapidly expanding, yet it remains unclear whether social risk factors influence which youth receive these therapies. Objective: To examine whether food insecurity among youth with obesity is associated with prescription of obesity pharmacotherapy, including GLP-1 receptor agonists (GLP-1RA). Design/Methods: We conducted a cross-sectional analysis of electronic health records of 475 youth aged 12-21 years (mean 13.4 ± 1.0; 50% female) receiving tertiary care for obesity at an academic medical center in Massachusetts (1/1/23-6/30/25). Food insecurity was assessed using a validated 2-item screener included in routine clinical screening. Logistic regression estimated associations between food insecurity and prescription of any obesity-related pharmacotherapy (primary outcome) or any GLP-1RA (secondary outcome), adjusting for insurance, housing stability, transportation access, race/ethnicity (Model 2), and body mass index z-score (BMIz; Model 3). Results: Within this sample, 19% (n = 94) of youth screened positive for household food insecurity (Table 1). Individuals with food insecurity were more likely to be publicly insured (86% vs 65%, p< 0.001), identify as Hispanic (72% vs 51%, p < 0.001), and report housing insecurity (35% vs 17%, p = 0.0004). Participants with food insecurity had higher mean (SD) BMIz versus those without (2.6 [0.9] vs 2.3 [0.9], p = 0.01), and greater prevalence of Class II-III obesity (74% vs 58%, p = 0.004). Overall, 31% were prescribed any pharmacotherapy and 14% were prescribed GLP-1RA. In adjusted models, food insecurity was not associated with pharmacotherapy (aOR 0.71, 95% CI 0.39-1.27) or GLP-1RA (aOR 0.84, 95% CI 0.4, 1.75) (Table 2). Higher BMI-z predicted pharmacotherapy prescription (aOR 3.26, 95% CI 2.40-4.42), while insurance type was not associated with prescribing.
Conclusion(s): In this single-center analysis, food insecurity was not significantly associated with prescription of obesity pharmacotherapy or GLP-1RA, although it was associated with increased severity of obesity. These findings highlight the importance of understanding the unique needs in supporting youth with food insecurity who are prescribed obesity pharmacotherapy to ensure equitable access and that health inequities are not further widened.
Table 1: Demographics by Food Security Status
Table 2: Association of food insecurity (exposure) with obesity pharmacotherapy (outcome)
Table 3: Multivariate Logistic Regression of Obesity Pharmacotherapy and Food Insecurity

 photo")
.jpg)
