Session: Technology 3: Telemedicine and Virtual Health
194 - Impact of a Virtual Maternity and Newborn Program Engagement on NICU Average Length of Stay in Rural Residents
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4191.194
Lena Bertozzi, Pomelo Care, New York, NY, United States; Ian J. Hooley, Pomelo Care, New York, NY, United States; Isabelle von Kohorn, Pomelo Care, Washington, DC, United States; Stacey Kallem, Pomelo Care, Merion Station, PA, United States; Sara Handley, Childrens Hospital of Philadelphia, Philadelphia, PA, United States
Head of Pediatrics Pomelo Care Merion Station, Pennsylvania, United States
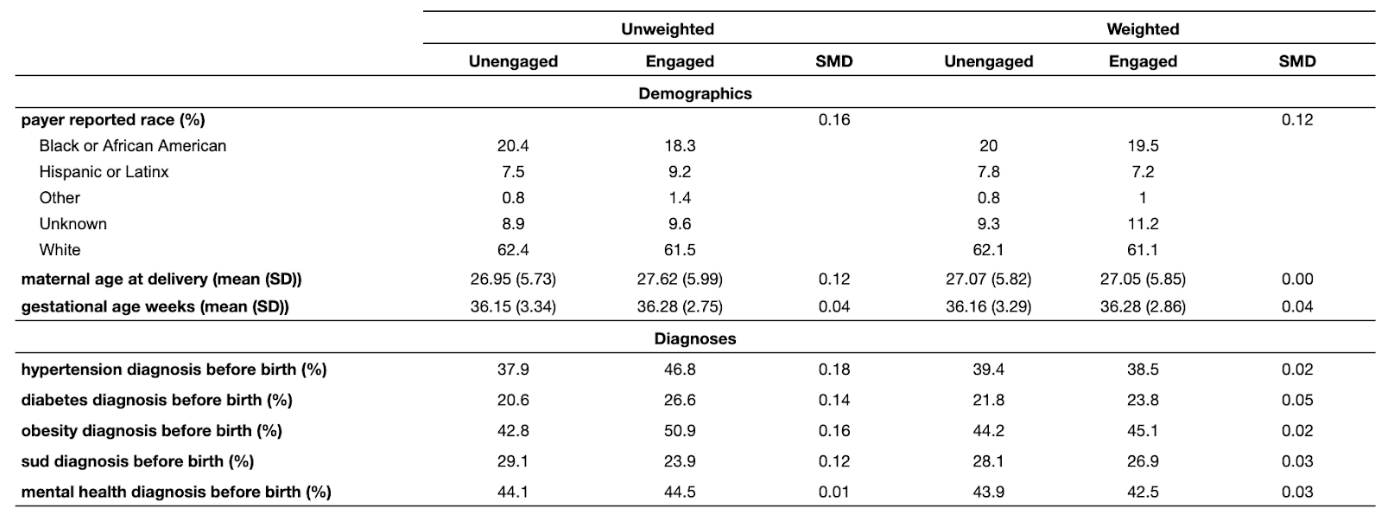
Background: Rural maternal-infant dyads face significant barriers to accessing care and experience worse outcomes. Utilizing virtual perinatal care models that provide 24/7 comprehensive virtual maternity care, specialized support during the Newborn Intensive Care Unit (NICU) stay, and assistance with transitions home may improve care and outcomes for these vulnerable dyads, representing a scalable model to address these disparities. Objective: To determine the association of engagement with a 24/7 virtual maternity and newborn program with NICU Average Length of Stay (ALOS) among infants of rural-residing, Medicaid and commercially-enrolled parents. Design/Methods: This retrospective cohort analysis included 1,258 infants admitted to a NICU between 01/01/2024 and 07/31/2025. Parents were categorized as rural-residing if they lived in a rural county based on Urban Influence Codes (i.e. 2,3,5,6,7,8, or 9). The primary exposure was defined as engagement with the virtual maternity and newborn program beginning at least one month before the infant's birth date. We assessed the program's effect on NICU ALOS utilizing regression analysis with Inverse Probability Weighting (IPW) to control for potential confounding variables. Risk adjustment variables included demographic characteristics, insurance coverage history, medical risk, and gestational age at birth. Any remaining imbalance was adjusted for with double-robust regressions. Results: Higher rates of advanced maternal age, hypertension, diabetes, and obesity in the program engaged group, and higher rates of substance use disorder in the unengaged group, were successfully weighted to achieve balance (standard mean difference < 0.1). Engagement with the virtual program was associated with a significant 2.2 day reduction in NICU ALOS (13.7%, p< 0.05) among the rural cohort.
Conclusion(s): Engagement with a virtual maternity and newborn program is associated with a statistically significant reduction in NICU ALOS for infants of parents residing in rural areas. This highlights the potential for accessible virtual care, providing both preventive prenatal and specialized NICU support, to improve outcomes and address healthcare disparities for high-risk infant populations.
Table 1: Subset of Unweighted and Weighted Risk Adjustment Variables of Engaged and Unengaged Populations

 photo")
.png)
