Session: Neonatal Hemodynamics and Cardiovascular Medicine 1
459 - Two-year outcomes of a randomized controlled trial of nonintervention versus oral ibuprofen for patent ductus arteriosus in premature infants
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3444.459
Seung Hyun Kim, Samsung Medical Center, Seoul, Seoul-t'ukpyolsi, Republic of Korea; So Yoon Ahn, Samsung Medical Center, SEOUL, Seoul-t'ukpyolsi, Republic of Korea; Yun Sil Chang, Sungkyunkwan university, Seoul, Seoul-t'ukpyolsi, Republic of Korea; Se In Sung, Samsung Medical Center, Seoul, Seoul-t'ukpyolsi, Republic of Korea
Hospital fellow Samsung Medical Center Seoul, Seoul-t'ukpyolsi, Republic of Korea
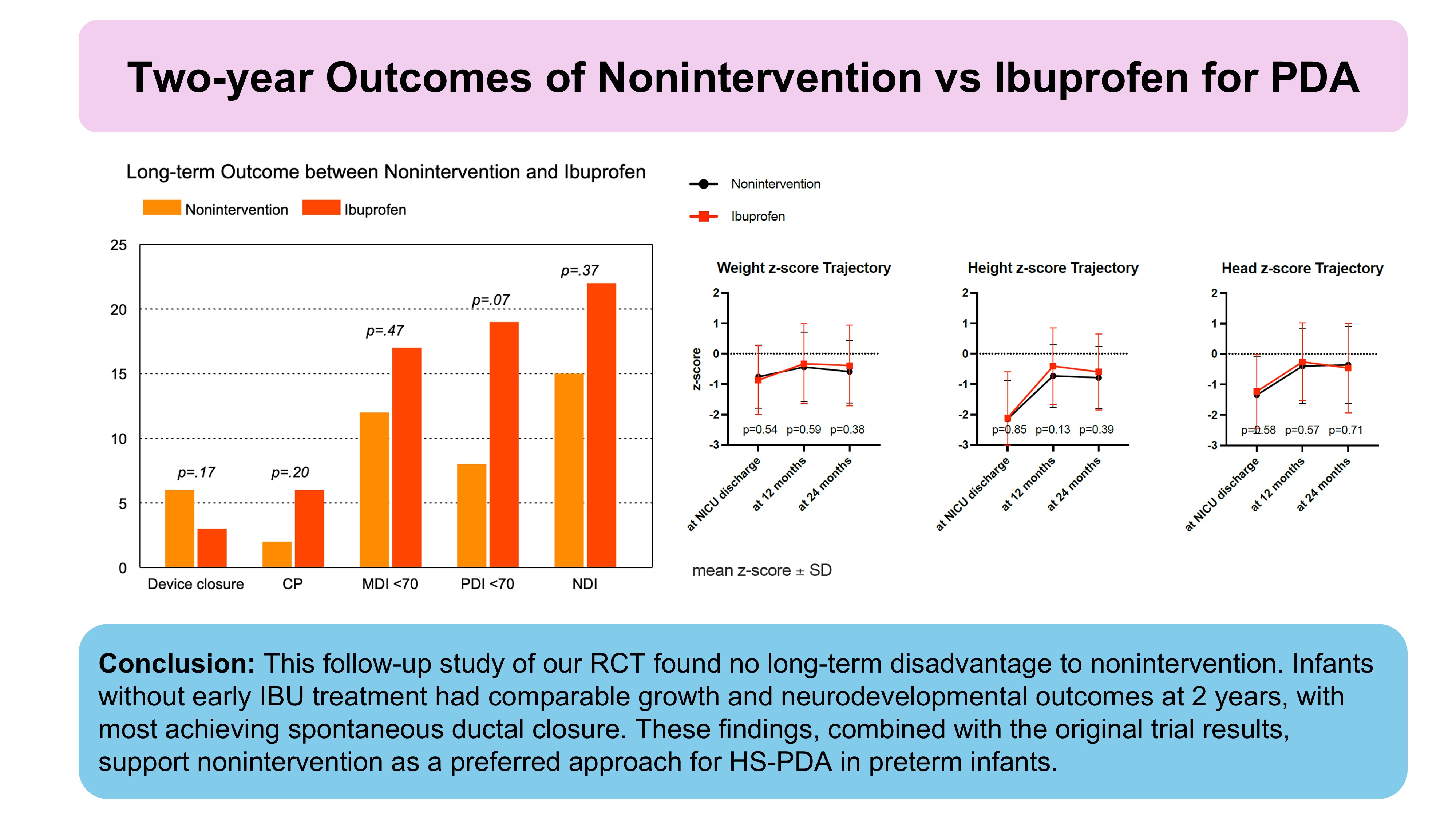
Background: Optimal management of patent ductus arteriosus (PDA) in premature infants remains debated, and the long-term impact of different strategies has not been well studied. We previously conducted a randomized clinical trial comparing nonintervention (NI) and oral ibuprofen (IBU) for hemodynamically significant PDA in preterm infants, which showed no significant difference in bronchopulmonary dysplasia or death during hospitalization. Objective: In this study, we aimed to present a prespecified longitudinal follow-up investigation to assess the outcomes of persistently open PDA at discharge, as well as growth and neurodevelopmental outcomes at 2 years' corrected age (CA), based on PDA management strategy. Design/Methods: Surviving infants from the original trial were evaluated at 2 years' CA. Examiners blinded to the management group assessed spontaneous ductal closure after hospital discharge, growth parameters, and neurodevelopmental outcomes. This longitudinal follow-up study was based on our previously published randomized clinical trial that compared NI with oral IBU for the management of hemodynamically significant PDA in preterm infants. The original double-blind, placebo-controlled trial enrolled 146 infants born at 23-30 weeks' gestational age with hemodynamically significant PDA (ductal size >1.5 mm with respiratory support requirement) diagnosed between postnatal days 6-14. Results: Among 130 survivors, open PDA at discharge was present in 7/66 (11%) NI and 2/64 (3%) IBU infants; spontaneous closure occurred in 3/7 NI infants but 0/2 IBU infants. Device closure occurred in 6% (4/66) of the NI group and 3% (2/64) of the IBU group (P=0.68) by 2 years' CA. Growth parameters-height, weight, and head circumference-did not differ significantly between groups. Neurodevelopmental impairment-defined as cerebral palsy, hearing or visual loss, or a Bayley Scales of Infant Development II mental or psychomotor development index below 70-was present in 15% (10/66) of the NI group and 22% (14/64) of the IBU group (P = 0.37).
Conclusion(s): This follow-up study demonstrated that NI for hemodynamically significant PDA in preterm infants resulted in growth and neurodevelopmental outcomes at 2 years' CA similar to those seen with IBU treatment. The high rate of spontaneous PDA closure and lack of significant differences in long-term morbidities support the safety of NI and raise questions about the benefit of routine pharmacologic closure.