Associate Principal Vizient Inc Hinsdale, Illinois, United States
Background: Firearm injuries are the leading cause of death among U.S. children and adolescents. Intent-whether self-harm, assault, accidental, or undetermined-is a major determinant of injury outcome. However, few studies have evaluated how developmental age modifies the relationship between intent and in-hospital mortality, limiting the precision of pediatric prevention and trauma response strategies. Objective: To assess predictors of in-hospital mortality among firearm-injured pediatric patients ( < 18 years), focusing on the interaction between age group and firearm injury intent. Design/Methods: This retrospective study used data from the Vizient Clinical Data Base, encompassing >1,350 hospitals nationwide (2019-2024). Pediatric inpatient and emergency department discharges with firearm injury ICD-10-CM codes (n=18,127) were analyzed using multivariable logistic regression. Covariates included race/ethnicity, sex, payer, social vulnerability (Vizient Vulnerability Index™), mental health and substance use disorders, and state Child Access Prevention (CAP) laws. The primary outcome was in-hospital or ED mortality. Results: The interaction between age and intent was significant (Wald χ² = 40.27, p < .0001).
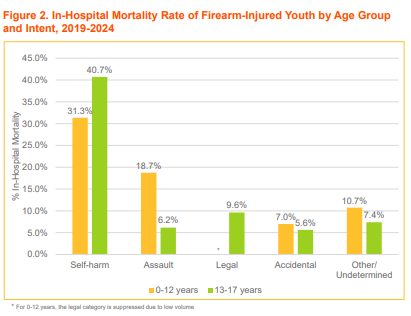
Children (0-12 years) had greater odds of death from assault and accidental firearm injuries than adolescents (13-17 years).
Self-harm injuries carried the highest mortality risk across both age groups.
Black (aOR=1.37) and "Other" race (aOR=2.76) youth had higher mortality risk versus White youth.
Female sex (aOR=0.80) and residence in higher-vulnerability communities (aOR=0.68) were associated with lower odds of death.
Youth in states without CAP laws had greater mortality risk (aOR=1.17, 95% CI 1.03-1.32).
Conclusion(s): Age meaningfully modifies the impact of intent on firearm mortality in pediatric patients. These findings support an age-intent model of firearm injury, which recognizes that the pathways and lethality of firearm exposure differ across developmental stages. Integrating this framework can enhance the targeting of age-appropriate prevention (e.g., CAP enforcement for young children, suicide prevention for teens) and age-tailored trauma care protocols. An age-intent model moves beyond "one-size-fits-all" firearm injury prevention, offering a developmental lens for pediatric policy and clinical action. Such stratification could guide trauma system design, anticipatory guidance, and risk communication to better protect children at different life stages.
Figure 1. Forest Plot of Adjusted Odds of In-Hospital Mortality Among Firearm-Injured Youth
In-Hospital Mortality Rate of Firearm-Injured Youth by Age Group and Intent, 2019-2024

.png)