623 - Administration of Donor Breast Milk (DBM), Necrotizing enterocolitis (NEC) and Mortality in Very Preterm (VPT, <33 weeks) or Very Low Birthweight Infants (VLBW, <1500 g)
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1600.623
Sujir P. Nayak, UTSW -Dallas, Dallas, TX, United States; Luc P. Brion, UT Southwestern Medical Center, FRISCO, TX, United States; Dimitrios Angelis, University of Texas Southwestern Medical School, Dallas, TX, United States; Cheryl Lair, University of Texas Southwestern Medical School, Dallas, TX, United States; Audrey Edwards, Parkland Health, Dallas, TX, United States; Steven Brown, Parkland Health, Dallas, TX, United States; Eric B. Ortigoza, UT Southwestern Medical Center, Dallas, TX, United States; Vonny Chong, University of Texas Southwestern Medical School, Dallas, TX, United States; Mambarambath A.. Jaleel, University of Texas Southwestern Medical School, Irving, TX, United States
Assistant Professor of Pediatrics UTSW -Dallas Dallas, Texas, United States
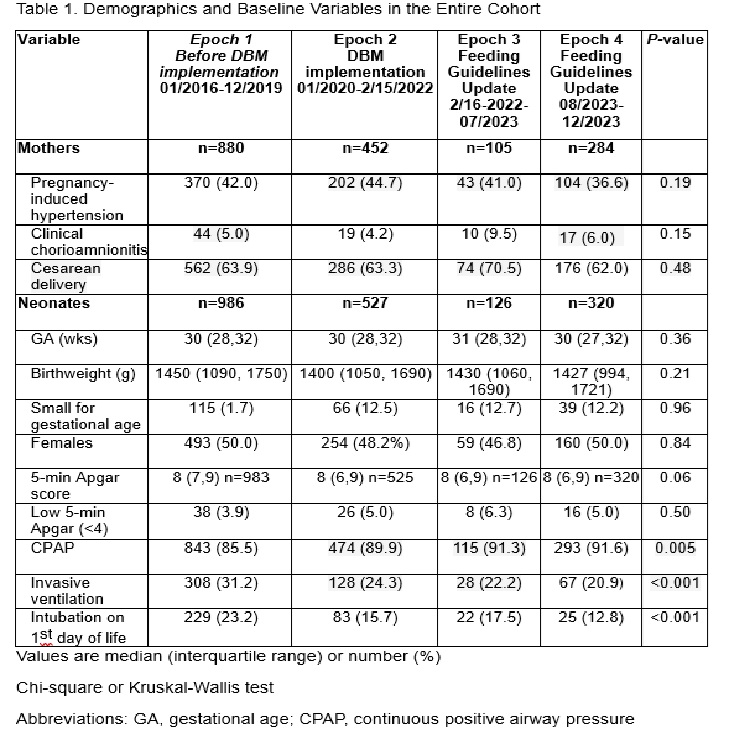
Background: : NEC is most frequent among VPT and VLBW infants. Systematic reviews have shown that feeding human milk instead of formula reduces the risk of NEC. A DBM Program was implemented in Parkland Health and Hospital System (PHHS) hospital in January 2020 as part of the NEC quality improvement initiative Objective: To assess the relationship between administration of DBM, duration of mother's own milk (MoM) feeding, NEC, and mortality in VPT and VLBW infants Design/Methods: This retrospective cohort study of VPT and VLBW infants was conducted at PHHS from 2016-2023, divided into 4 epochs. Infants on comfort care only, with severe congenital anomalies or never fed enterally were excluded. Variables extracted from electronic health records were entered into stepwise logistic regression analyses to test their association with NEC stage ≥II, III and mortality. Among infants born after DBM implementation (2020-2023), the predicted likelihood of early DBM was obtained from logistic regression and used to establish individual propensity scores (PS) for early DBM initiation. Comparison of early DBM and controls was inversely weighted for individual PS using Augmented Inverse Probability Weight (AIPW). Outcomes were assessed by the adjusted average treatment effect (ATE), the bootstrap bias corrected ATE and the adjusted odds ratio (aOR) obtained from subsequent logistic regression analysis. Results: Among 1959 infants, 96 (4.9%) developed NEC stage ≥II, 46 (2.3%) NEC III and 61 (3.1%) died (Table 1). In the entire cohort, prolonged MoM feeding [until ≥34 wks postmenstrual age (PMA)] was independently associated with less NEC stage ≥II, III and mortality. Among infants born in 2020-2023, factors independently associated with early DBM feeding are listed in Table 2. PS matching in 832 infants minimized differences between the two groups for all variables associated with early DBM (Table 2) as well as for CPAP and invasive ventilation. On PS analysis early DBM feeding was associated with no change in NEC stage ≥II or III, but with more MoM feeding to ≥34 wks PMA and more delay in formula feeding to ≥ 34 weeks PMA. Early DBM feeding was associated with lower ATE and aOR in mortality to discharge but not with bootstrap corrected ATE (Table 3).
Conclusion(s): PS showed that early initiation of DBM was associated with no change in NEC but less MoM feeding to ≥34 wks PMA. Because MoM feeding to ≥34 wks PMA was associated with less NEC and mortality in the entire cohort, current efforts are focused on increasing and prolonging MoM feeding in VLBW and VPT infants
Table 1: Demographics and Baseline Variables in the Entire Cohort
Table 2: PS Matching Treated (Early DBM 1st 2 days) vs Controls among Infants born in 2020-2023: Variables associated with early DBM feeding
Table 3: Results of Propensity Score Analysis of DBM feeding within first 2 Days Postnatal among Infants born after DBM implementation (2020-2023)

.jpg)
.jpg)
