Session: Global Neonatal & Children's Health Trainee Ongoing Projects
TOP 21 - Assessing the Delivered Pressure of Low-Cost Bubble Continuous Positive Airway Pressure Among Neonates in Low Resource Settings
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1781.TOP 21
Tolulope Oshiba-Fowode, University of Minnesota, Minneapolis, MN, United States; Patience Ungut. Kanhu, JOS UNIVERSITY TEACHING HOSPITAL, JOS PLATEAU STATE, JOS, Plateau, Nigeria; Bose Toma, Jos University Teaching Hospital, Jos, Plateau, Nigeria; Anne M. White, University of Minnesota Medical School, Minneapolis, MN, United States; Aderonke Gbadebo, University of Minnesota Medical School, Minneapolis, MN, United States; Andrew Wu, Hennepin County Medical Center, Minneapolis, MN, United States; Ashley Bjorklund, Hennepin County Medical Center and University of Minnesota, MInneapolis, MN, United States; Jennifer Udeogu, Baylor College of Medicine, Houston, TX, United States; Jared Floersch, University of Minnesota, Minneapolis, MN, United States; Molly Gardner, University of Minnesota Medical School, Ely, MN, United States; Kachollom G. Bot, Jos university teaching hospital, Jos, Plateau, Nigeria; Udochukwu Michael. Diala, Jos University Teaching Hospital, Jos, Plateau, Nigeria; Tina Slusher, University of Minnesota, Minneapolis, MN, United States
Resident University of Minnesota Minneapolis, Minnesota, United States
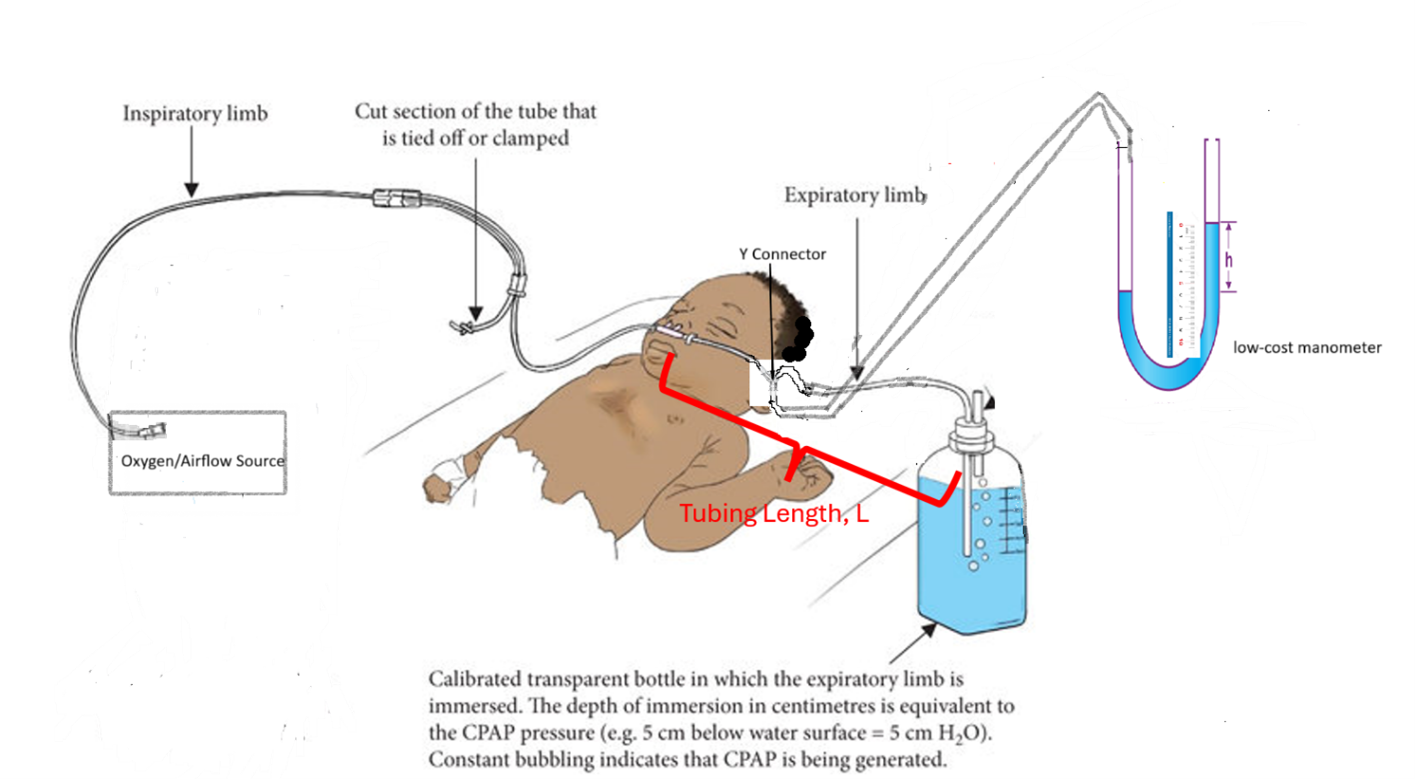
Background: Bubble Continuous Positive Airway Pressure (bCPAP) has become a widely adopted, cost-effective intervention for neonatal respiratory distress syndrome (RDS) in low-resource settings (LRSs). By providing effective non-invasive respiratory support for RDS, bCPAP has the potential to safely reduce neonatal mortality rates in LRSs around the world. Improper configuration or use of bCPAP systems can result in inadequate or excessive positive pressures, increasing the risk of complications such as insufficient respiratory support or pneumothorax. As such, the improvised or modified devices, though addressing immediate resource shortages, are also prone to delivering inconsistent or unpredictable pressures, highlighting the importance of standardized equipment, rigorous training, and ongoing monitoring. Although studies have posited the safety of the low cost bCPAP, there has recently been specific concern raised about unsafe, high-pressure inadvertently being delivered to neonates with low-cost bCPAP; this has motivated the current project, which aims to objectively measure the estimated pressure delivered by bCPAP systems to better quantify the risk with a modified low-cost circuit in resource-limited settings. Objective: To determine the estimated pressure in the circuit of a neonate on low-cost bubble continuous positive airway pressure (bCPAP) therapy by utilizing a low-cost manometer. Design/Methods: Bench testing was conducted on modified low-cost bCPAP setups commonly used in neonatal units across LMICs. Using an in-line manometer, pressures were measured across a range of oxygen flow rates (4-8 L/min), water column depths (5-8 cm H₂O), and circuit configurations designed to simulate typical bedside conditions. Three nasal cannula types were tested: Salter Labs infant, Hudson pediatric, and Hudson adult cannulas. Each setup used a Y-connector placed ~20 cm from the nasal prongs. To simulate circuit leaks, blunt 18-gauge needles were inserted into one or both prongs of the sealed nasal cannulas. Pressure differences were measured based on fluid height changes, and calculations were based on the hydrostatic pressure formula: P = ρgh. All measurements were recorded, plotted, and analyzed to evaluate variability under different conditions. Following bench testing, a pilot study was conducted in a LMIC neonatal unit. Five neonates requiring non-invasive ventilation for respiratory distress were enrolled, and serial in-line pressure measurements were obtained using the same setup.
Figure 1: Generalized schema for setup of low-cost bCPAP and low-cost manometer.
Figure 2: Graphical representation of laboratory findings when varying oxygen flow-rate (in LPM) was plotted against measured (bCPAP in cmH20) with and without leaks

 photo")
.png)
